

Effect of antibiotic therapy on the density of vancomycin-resistant enterococci in the stool of colonized patients
- PMID: 11136263
- PMCID: PMC4370337
- DOI: 10.1056/NEJM200012283432604
Effect of antibiotic therapy on the density of vancomycin-resistant enterococci in the stool of colonized patients
Abstract
Background: Colonization and infection with vancomycin-resistant enterococci have been associated with exposure to antibiotics that are active against anaerobes. In mice that have intestinal colonization with vancomycin-resistant enterococci, these agents promote high-density colonization, whereas antibiotics with minimal antianaerobic activity do not.
Methods: We conducted a seven-month prospective study of 51 patients who were colonized with vancomycin-resistant enterococci, as evidenced by the presence of the bacteria in stool. We examined the density of vancomycin-resistant enterococci in stool during and after therapy with antibiotic regimens and compared the effect on this density of antianaerobic agents and agents with minimal antianaerobic activity. In a subgroup of 10 patients, cultures of environmental specimens (e.g., from bedding and clothing) were obtained.
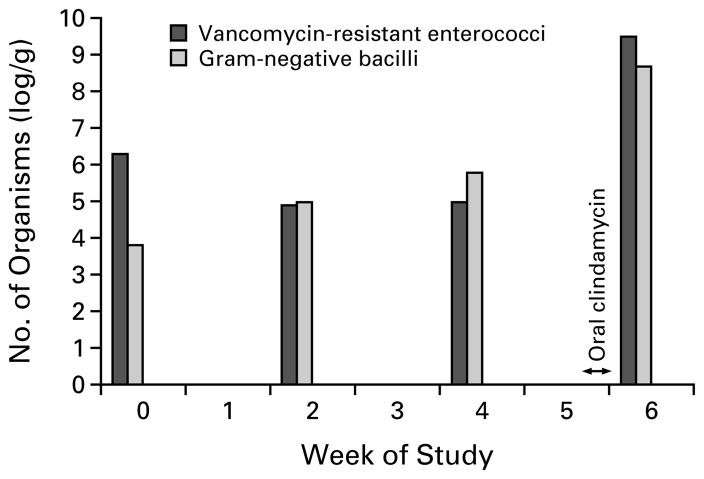
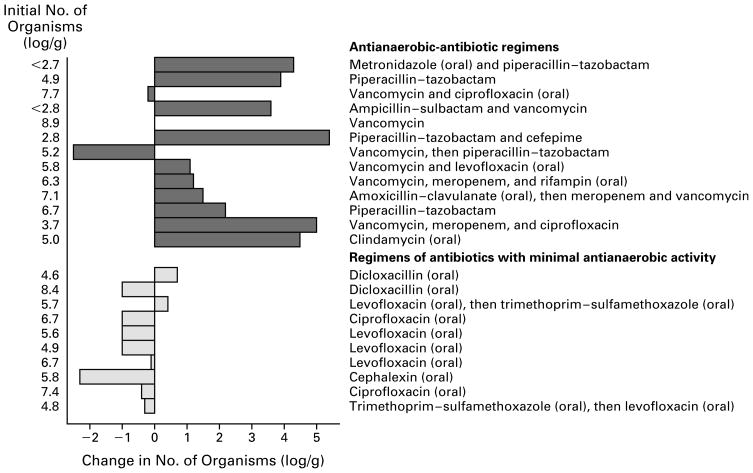
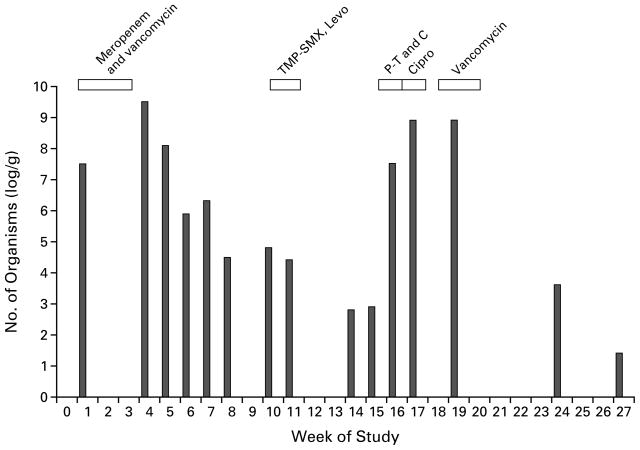
Results: During treatment with 40 of 42 antianaerobic-antibiotic regimens (95 percent), high-density colonization with vancomycin-resistant enterococci was maintained (mean [+/-SD] number of organisms, 7.8+/-1.5 log per gram of stool). The density of colonization decreased after these regimens were discontinued. Among patients who had not received antianaerobic antibiotics for at least one week, 10 of 13 patients who began such regimens had an increase in the number of organisms of more than 1.0 log per gram (mean increase, 2.2 log per gram), whereas among 10 patients who began regimens of antibiotics with minimal antianaerobic activity, there was a mean decrease in the number of enterococci of 0.6 log per gram (P=0.006 for the difference between groups). When the density of vancomycin-resistant enterococci in stool was at least 4 log per gram, 10 of 12 sets of cultures of environmental specimens had at least one positive sample, as compared with 1 of 9 sets from patients with a mean number of organisms in stool of less than 4 log per gram (P=0.002).
Conclusions: For patients with vancomycin-resistant enterococci in stool, treatment with antianaerobic antibiotics promotes high-density colonization. Limiting the use of such agents in these patients may help decrease the spread of vancomycin-resistant enterococci.
Figures
Comment in
-
Managing antibiotic resistance.N Engl J Med. 2000 Dec 28;343(26):1961-3. doi: 10.1056/NEJM200012283432610. N Engl J Med. 2000. PMID: 11136269 No abstract available.
References
-
- Morris JG, Shay DK, Hebden JN, et al. Enterococci resistant to multiple antimicrobial agents, including vancomycin: establishment of endemicity in a university medical center. Ann Intern Med. 1995;123:250–9. - PubMed
-
- Shay DK, Maloney SA, Montecalvo M, et al. Epidemiology and mortality risk of vancomycin-resistant enterococcal bloodstream infections. J Infect Dis. 1995;172:993–1000. - PubMed
-
- Beezhold DW, Slaughter S, Hayden MK, et al. Skin colonization with vancomycin-resistant enterococci among hospitalized patients with bacteremia. Clin Infect Dis. 1997;24:704–6. - PubMed
-
- Handwerger S, Raucher B, Altarac D, et al. Nosocomial outbreak due to Enterococcus faecium highly resistant to vancomycin, penicillin, and gentamicin. Clin Infect Dis. 1993;16:750–5. - PubMed
-
- Moreno F, Grota P, Crisp C, et al. Clinical and molecular epidemiology of vancomycin-resistant Enterococcus faecium during its emergence in a city in southern Texas. Clin Infect Dis. 1995;21:1234–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical