

Switching between intravenous and oral pantoprazole
- PMID: 11154164
- PMCID: PMC6746342
- DOI: 10.1097/00004836-200101000-00007
Switching between intravenous and oral pantoprazole
Abstract
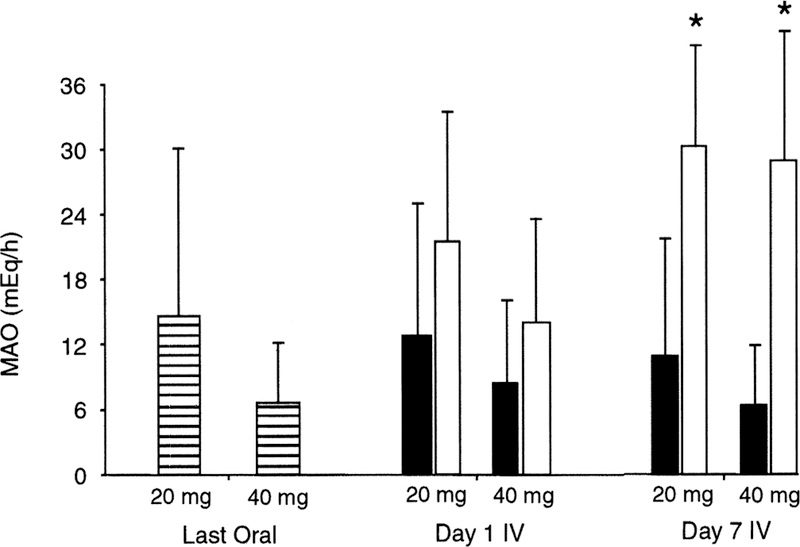
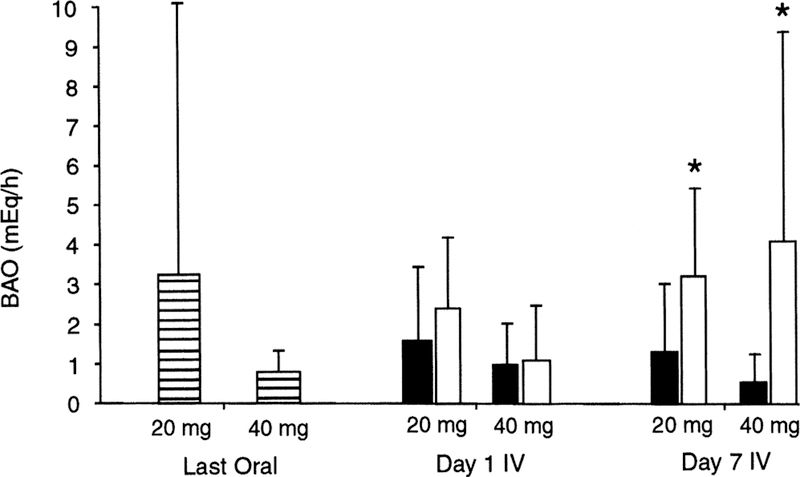
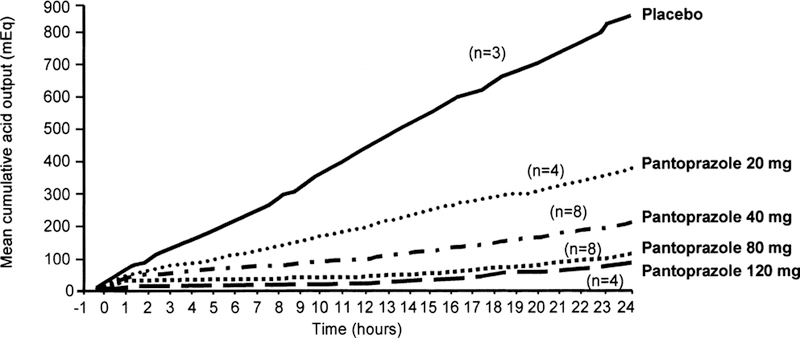
Proton pump inhibitors (PPIs) are the most effective antisecretory drugs available for controlling gastric acid acidity and volume. They are the drugs of choice in the treatment of moderate-to-severe gastroesophageal reflux disease, hypersecretory disorders, and peptic ulcers. Currently in the United States, they are only available in an oral formulation. However, pantoprazole will soon be available in an intravenous formulation and will extend the power of PPIs to inpatient hospital settings. Intravenous pantoprazole has been shown to be effective and safe in clinical trials. Intravenous pantoprazole is indicated for the treatment of patients who require PPI therapy but who are unable to take oral medication. Intravenous pantoprazole has been shown to maintain acid suppression in patients switched from oral PPIs, so no change in dosage is required when switching from one formulation to the other. Potential hospital-based uses for intravenous PPI therapy include perioperative use as prophylaxis for acid aspiration syndrome during induction of anesthesia, prophylaxis for stress-related mucosal disease, and management of gastrointestinal bleeding from stress or acid peptic disease.
Figures
Similar articles
-
Evaluation of omeprazole, lansoprazole, pantoprazole, and rabeprazole in the treatment of acid-related diseases.J Am Pharm Assoc (Wash). 2000 Jan-Feb;40(1):52-62; quiz 121-3. doi: 10.1016/s1086-5802(16)31036-1. J Am Pharm Assoc (Wash). 2000. PMID: 10665250 Review.
-
Replacement of oral proton pump inhibitors with intravenous pantoprazole to effectively control gastric acid hypersecretion in patients with Zollinger-Ellison syndrome.Am J Gastroenterol. 2001 Dec;96(12):3274-80. doi: 10.1111/j.1572-0241.2001.05325.x. Am J Gastroenterol. 2001. PMID: 11774936
-
Oral and intravenous dosage forms of pantoprazole are equivalent in their ability to suppress gastric acid secretion in patients with gastroesophageal reflux disease.Am J Gastroenterol. 2000 Mar;95(3):626-33. doi: 10.1111/j.1572-0241.2000.01834.x. Am J Gastroenterol. 2000. PMID: 10710049 Clinical Trial.
-
Efficacy and safety of pantoprazole in patients with gastroesophageal reflux disease using an intravenous-oral regimen. Austrian Intravenous Pantoprazole Study Group.Hepatogastroenterology. 1999 May-Jun;46(27):1809-15. Hepatogastroenterology. 1999. PMID: 10430350 Clinical Trial.
-
Pantoprazole: an update of its pharmacological properties and therapeutic use in the management of acid-related disorders.Drugs. 2003;63(1):101-33. doi: 10.2165/00003495-200363010-00006. Drugs. 2003. PMID: 12487624 Review.
Cited by
-
Reducing gastric secretions--a role for histamine 2 antagonists or proton pump inhibitors in malignant bowel obstruction?Support Care Cancer. 2009 Dec;17(12):1463-8. doi: 10.1007/s00520-009-0609-3. Epub 2009 Mar 17. Support Care Cancer. 2009. PMID: 19290549
-
Effect of pantoprazole and its interactions with vecuronium on the neuromuscular junction.Indian J Pharmacol. 2010 Feb;42(1):36-9. doi: 10.4103/0253-7613.62410. Indian J Pharmacol. 2010. PMID: 20606835 Free PMC article.
-
Stress-related Mucosal Disease.Curr Treat Options Gastroenterol. 2003 Apr;6(2):135-145. doi: 10.1007/s11938-003-0014-9. Curr Treat Options Gastroenterol. 2003. PMID: 12628072
References
-
- Long RG. Reflux oesophagitis and its treatment. Br J Clin Pract Symp Suppl 1994;75:36–40. - PubMed
-
- DeVault KR, Castell DO. Guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Arch Intern Med 1995;155:2165–73. - PubMed
-
- Graham DY, Smith JL, Patterson DJ. Why do apparently healthy people use antacid tablets? Am J Gastroenterol 1983;78:257–60. - PubMed
-
- Fass R, Hixson LJ, Ciccolo ML, et al. Contemporary medical therapy for gastroesophageal reflux disease. Am Fam Physician 1997;55:205–12. - PubMed
-
- Richter JE. Long-term management of gastroesophageal reflux disease and its complications. Am J Gastroenterol 1997;92:30S–5S. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
