

Endoscopic mucosal resection for treatment of early gastric cancer
- PMID: 11156645
- PMCID: PMC1728193
- DOI: 10.1136/gut.48.2.225
Endoscopic mucosal resection for treatment of early gastric cancer
Abstract
Background: In Japan, endoscopic mucosal resection (EMR) is accepted as a treatment option for cases of early gastric cancer (EGC) where the probability of lymph node metastasis is low. The results of EMR for EGC at the National Cancer Center Hospital, Tokyo, over a 11 year period are presented.
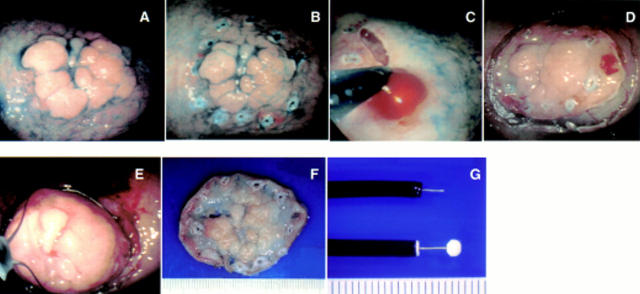
Methods: EMR was applied to patients with early cancers up to 30 mm in diameter that were of a well or moderately histologically differentiated type, and were superficially elevated and/or depressed (types I, IIa, and IIc) but without ulceration or definite signs of submucosal invasion. The resected specimens were carefully examined by serial sections at 2 mm intervals, and if histopathology revealed submucosal invasion and/or vessel involvement or if the resection margin was not clear, surgery was recommended.
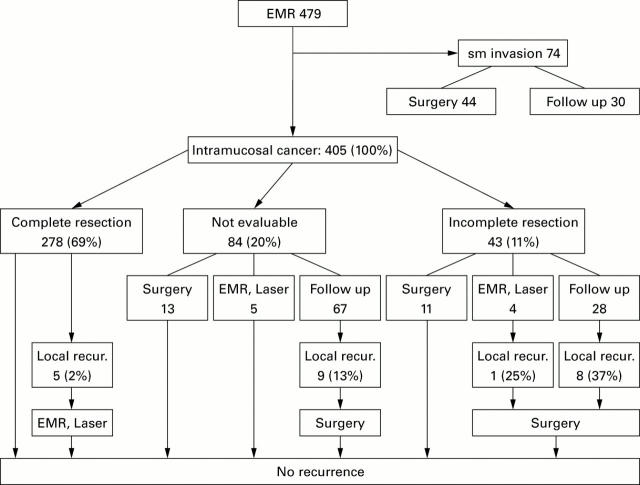
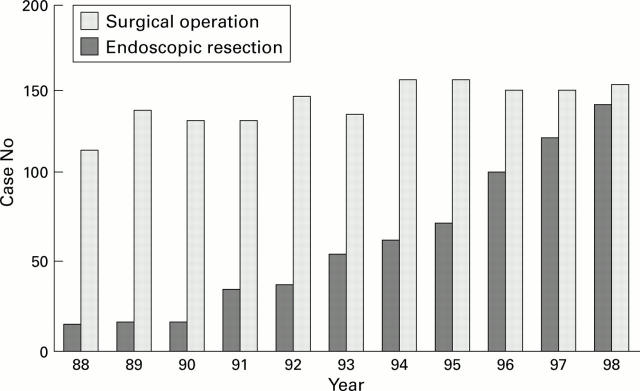
Results: Four hundred and seventy nine cancers in 445 patients were treated by EMR from 1987 to 1998 but submucosal invasion was found on subsequent pathological examination in 74 tumours. Sixty nine percent of intramucosal cancers (278/405) were resected with a clear margin. Of 127 cancers without "complete resection", 14 underwent an additional operation and nine were treated endoscopically; the remainder had intensive follow up. Local recurrence in the stomach occurred in 17 lesions followed conservatively, in one lesion treated endoscopically, and in five lesions with complete resection. All tumours were diagnosed by follow up endoscopy and subsequently treated by surgery. There were no gastric cancer related deaths during a median follow up period of 38 months (3-120 months). Bleeding and perforation (5%) were two major complications of EMR but there were no treatment related deaths.
Conclusion: In our experience, EMR allows us to perform less invasive treatment without sacrificing the possibility of cure.
Figures
Comment in
-
Endoscopic mucosal resection for early gastric cancer.Gut. 2001 Feb;48(2):151-2. doi: 10.1136/gut.48.2.151. Gut. 2001. PMID: 11156631 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical