

Relative contribution of resting haemodynamic profile and lung function to exercise tolerance in male patients with chronic heart failure
- PMID: 11156669
- PMCID: PMC1729632
- DOI: 10.1136/heart.85.2.179
Relative contribution of resting haemodynamic profile and lung function to exercise tolerance in male patients with chronic heart failure
Abstract
Objective: To clarify the relative contribution of resting haemodynamic profile and pulmonary function to exercise capacity in patients with heart failure.
Setting: Cardiology department and cardiac rehabilitation unit in a tertiary centre.
Design: 161 male patients (mean (SD) age 59 (9) years) with heart failure (New York Heart Association class II-IV, left ventricular ejection fraction 23 (7)%) underwent spirometry, alveolar capillary diffusing capacity (DLCO), and mouth inspiratory and expiratory pressures (MIP, MEP, respectively, in 100 patients). Right heart catheterisation and a symptom limited cardiopulmonary exercise test were performed in 137 patients within 3-4 days.
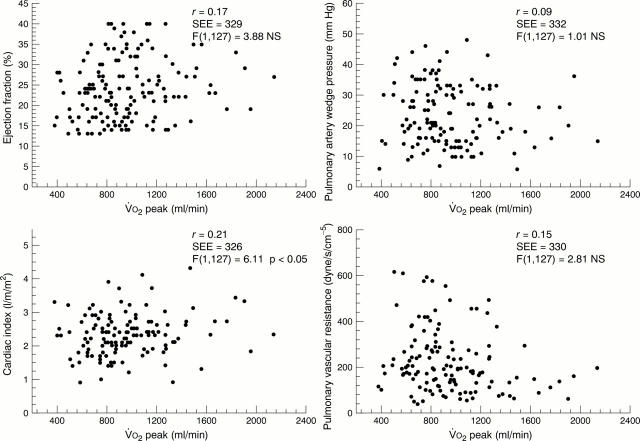
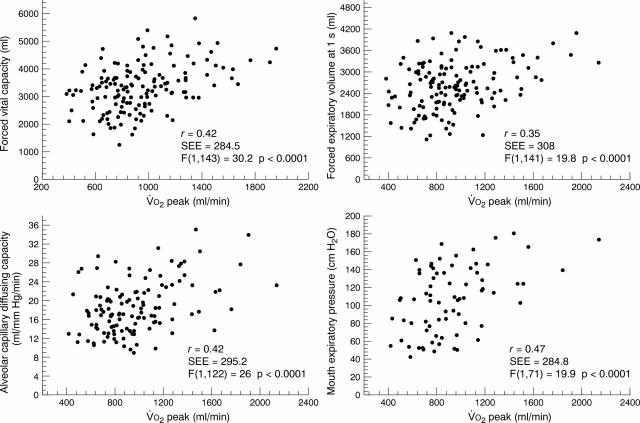
Results: Mean peak exercise oxygen consumption (VO(2)) was 13 (3.9) ml/kg/min. Among resting haemodynamic variables only cardiac index showed a significant correlation with peak VO(2). There were no differences in haemodynamic variables between patients with peak VO(2) </= or > 14 ml/kg/min. There was a moderate correlation (p < 0.05) between several pulmonary function variables and peak VO(2). Forced vital capacity (3.5 (0.9) v 3.2 (0.8) l, p < 0.05) and DLCO (21.6 (6.9) v 17.7 (5.5) ml/mm Hg/min, p < 0.05) were higher in patients with peak VO(2) > 14 ml/kg/min than in those with peak VO(2) </= 14 ml/kg/min. Using a stepwise regression analysis, the respiratory and haemodynamic variables which correlated significantly with peak VO(2) were DLCO, MEP, and cardiac index, with an overall R value of 0.63.
Conclusions: The data confirm previous studies showing a poor correlation between resting indices of cardiac function and exercise capacity in heart failure. However, several pulmonary function variables were related to peak exercise VO(2). In particular, lung diffusing capacity and respiratory muscle function seem to affect exercise tolerance during heart failure.
Figures
Similar articles
-
Pulmonary and peripheral vascular factors are important determinants of peak exercise oxygen uptake in patients with heart failure.J Am Coll Cardiol. 1993 Mar 1;21(3):641-8. doi: 10.1016/0735-1097(93)90096-j. J Am Coll Cardiol. 1993. PMID: 8436745
-
Pulmonary function, cardiac function, and exercise capacity in a follow-up of patients with congestive heart failure treated with carvedilol.Am Heart J. 1999 Sep;138(3 Pt 1):460-7. doi: 10.1016/s0002-8703(99)70148-1. Am Heart J. 1999. PMID: 10467196 Clinical Trial.
-
Resting lung function and hemodynamic parameters as predictors of exercise capacity in patients with chronic heart failure.Chest. 2003 May;123(5):1386-93. doi: 10.1378/chest.123.5.1386. Chest. 2003. PMID: 12740252
-
Peak VO2 in elderly patients with heart failure.Int J Cardiol. 2008 Apr 10;125(2):166-71. doi: 10.1016/j.ijcard.2007.10.004. Epub 2007 Dec 11. Int J Cardiol. 2008. PMID: 18067981 Review.
-
Exercise Intolerance in Heart Failure: Central Role for the Pulmonary System.Exerc Sport Sci Rev. 2020 Jan;48(1):11-19. doi: 10.1249/JES.0000000000000208. Exerc Sport Sci Rev. 2020. PMID: 31453845 Free PMC article. Review.
Cited by
-
Lung diffusion capacity in advanced heart failure: relation to central haemodynamics and outcome.ESC Heart Fail. 2019 Apr;6(2):379-387. doi: 10.1002/ehf2.12401. Epub 2019 Feb 19. ESC Heart Fail. 2019. PMID: 30784223 Free PMC article.
-
Predictors of Exercise Capacity in Dilated Cardiomyopathy with Focus on Pulmonary Venous Flow Recorded with Transesophageal Eco-Doppler.J Clin Med. 2021 Dec 18;10(24):5954. doi: 10.3390/jcm10245954. J Clin Med. 2021. PMID: 34945249 Free PMC article.
-
Echocardiography versus intracardiac electrocardiography-based optimization for cardiac resynchronization therapy : a comparative clinical long-term trial.Herz. 2011 Oct;36(7):592-9. doi: 10.1007/s00059-011-3507-7. Herz. 2011. PMID: 21922233 Clinical Trial.
-
Levosimendan improves calcium sensitivity of diaphragm muscle fibres from a rat model of heart failure.Br J Pharmacol. 2011 Feb;162(3):566-73. doi: 10.1111/j.1476-5381.2010.01048.x. Br J Pharmacol. 2011. PMID: 20880026 Free PMC article.
-
Oxygen uptake kinetics in chronic heart failure: clinical and physiological aspects.Neth Heart J. 2009 Jun;17(6):238-44. doi: 10.1007/BF03086254. Neth Heart J. 2009. PMID: 19789686 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical