

Utility of balloon-assisted Guglielmi detachable coiling in the treatment of 49 cerebral aneurysms: a retrospective, multicenter study
- PMID: 11156781
- PMCID: PMC7973939
Utility of balloon-assisted Guglielmi detachable coiling in the treatment of 49 cerebral aneurysms: a retrospective, multicenter study
Abstract
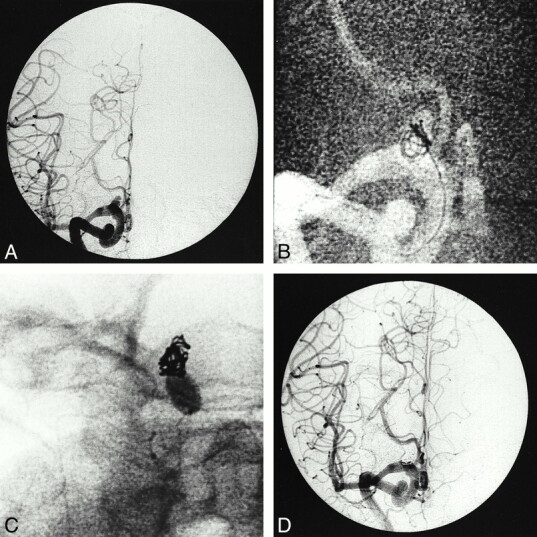
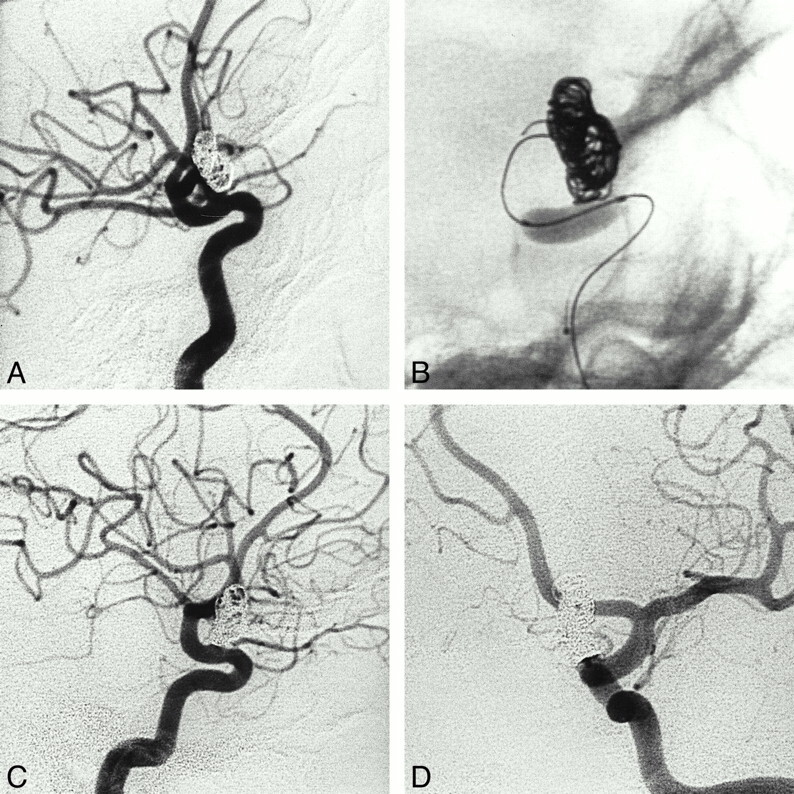
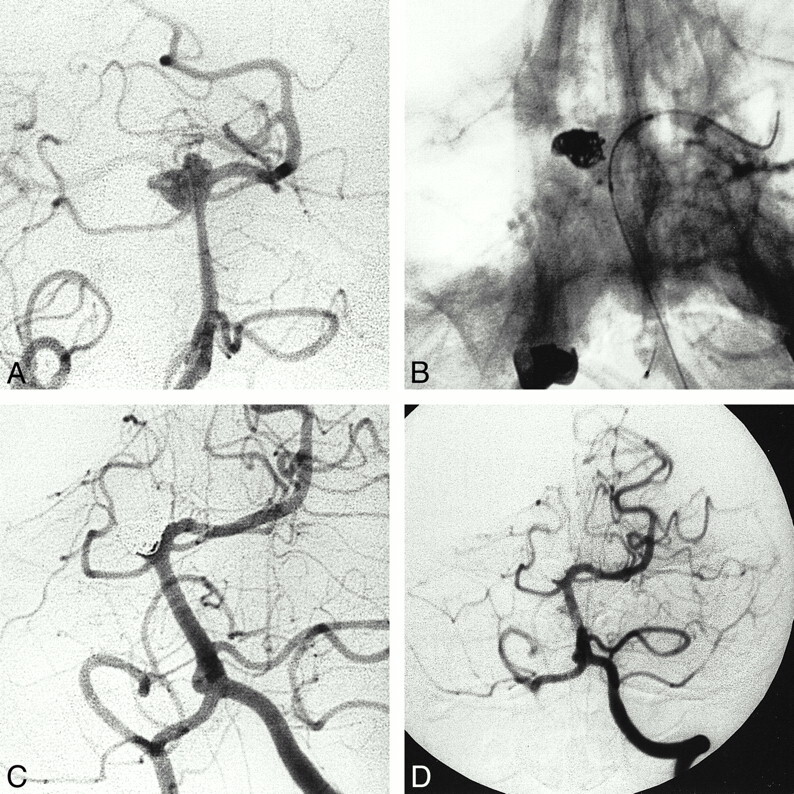
Background and purpose: The management of wide-necked aneurysms or aneurysms with a neck-to-body ratio close to 1 is a difficult challenge for the interventional radiologist because of the risk of coil migration or coil protrusion into the parent vessel. Our objective was to evaluate the efficacy and safety of balloon-assisted coiling as well as the follow-up results of occlusion for those difficult aneurysms in which conventional treatment with Guglielmi detachable coils (GDCs) had failed.
Methods: A nondetachable balloon was used in 49 procedures performed in 44 patients (35 women and nine men) who underwent GDC coiling of aneurysms. Every aneurysm had either a wide neck or a sac diameter/neck size ratio (SNR) of 1.5 or less.
Results: In four (8%) of the procedures, balloon placement failed, leaving a total of 45 aneurysms treated with balloon-assisted coiling. Final results consisted of total occlusion in 30 cases (67%), subtotal occlusion in 11 cases (24%), and incomplete occlusion in four cases (9%). We found a correlation between the diameter of the sac and the occlusion rate, but not between the size of the neck or the SNR and the occlusion rate. Two thromboembolic complications occurred, but neither had clinical consequences. No aneurysmal rupture was observed during treatment. Final angiographic follow-up time ranged from 3 months to 5 years (mean, 16 months).
Conclusion: Balloon-assisted coiling is an important adjunct in the treatment of aneurysms with a wide neck or low SNR. In our experience, this technique allowed safe and efficient treatment of aneurysms when conventional GDC treatment had failed.
Figures
References
-
- Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, 1: electrochemical basis, technique and experimental results. J Neurosurg 1991;75:1-7 - PubMed
-
- Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, 2: preliminary clinical experience. J Neurosurg 1991;75:8-14 - PubMed
-
- Nichols DA, Meyer FB, Piepgras DG, Smith PL. Endovascular treatment of intracranial aneurysms: subject review. Mayo Clin Proc 1994;69:272-285 - PubMed
-
- Richling B, Bazinsky G, Gross C, Gruber A, Killer M. Early clinical outcome of patients with ruptured cerebral aneurysms treated by endovascular (G.D.C.) or micro surgical techniques: a single center experience. Intervent Neuroradiol 1995;1:19-27 - PubMed
-
- McDougall CG, Halbach VV, Dowd CF, Higashida RT, Larsen DW, Hieshima GB. Endovascular treatment of basilar tip aneurysms using electrolytically detachable coils. J Neurosurg 1996;84:393-399 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical