

Review
Percutaneous vertebroplasty: a developing standard of care for vertebral compression fractures
Affiliations
- PMID: 11156786
- PMCID: PMC7973930
Item in Clipboard
Review
Percutaneous vertebroplasty: a developing standard of care for vertebral compression fractures
AJNR Am J Neuroradiol.
2001 Feb.
No abstract available
Figures
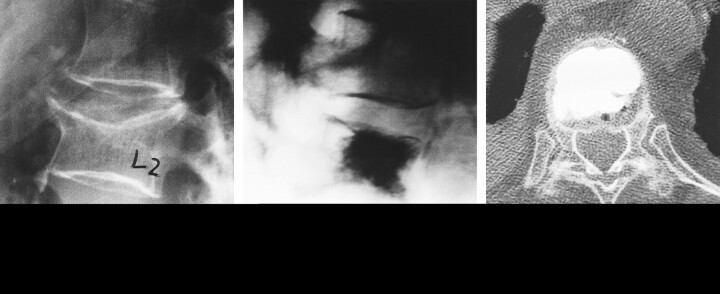
Typical osteoporotic VCF at L2. A, Preoperative radiograph, lateral view. B, Radiograph after treatment with vertebroplasty. The dark area represents PMMA opacified with barium sulfate. C, Axial CT scan of the treated L2 segment.
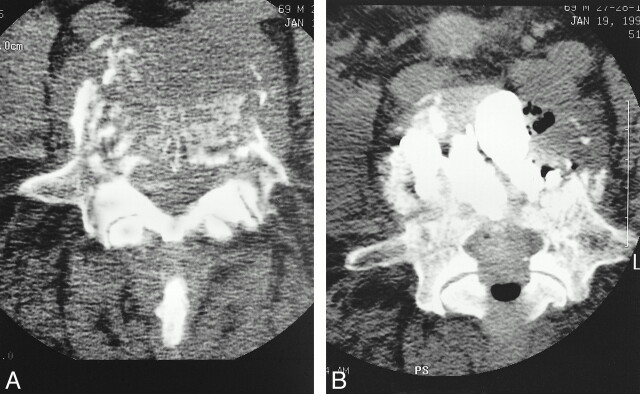
A and B, Pre- (A) and postoperative (B) axial CT studies in a patient with an L5 vertebra destroyed by renal cell carcinoma who experienced pain relief 24 hours after PVP (which filled much of the vertebra with PMMA)
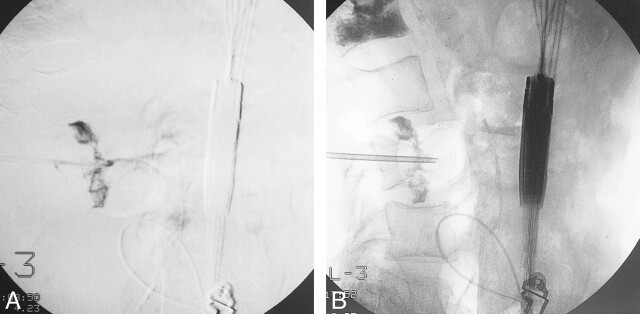
Venographic studies of an osteoporotic VCF. A, Lateral digital subtraction venogram shows nonionic radiographic contrast material leaking into both adjacent disks through endplate fractures. B, Lateral venogram without digital subtraction of the same site, obtained approximately 10 minutes after A. Note that the radiographic contrast agent is still apparent and thus may have impeded visualization of possible cement leaks during PVP.
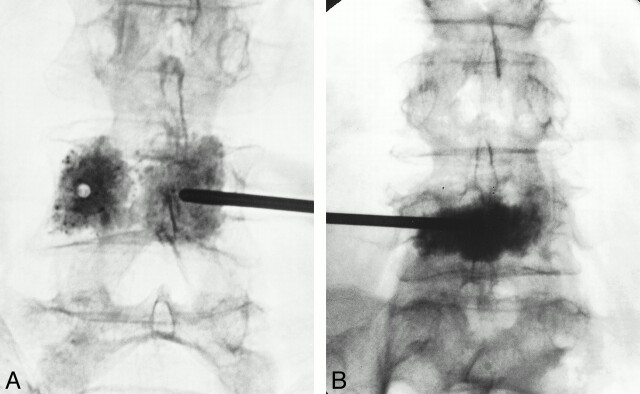
Injection techniques. A, Anterolateral radiograph shows vertebroplasty performed via a bipedicular approach and injections.B, Anterolateral radiograph shows vertebroplasty performed via a single parapedicular approach, which resulted in a central needle position and good filling with one injection of cement
References
-
- Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG. Methylmethacrylate as an adjunct in internal fixation of pathological fractures: experience with three hundred and seventy-five cases. J Bone Joint Surg 1976;58A:1047-1055 - PubMed
-
- Sundaresan N, Galicich JH, Lane JM, Bains MS, Mc Cormack P. Treatment of neoplastic epidural cord compression by vertebral body resection and stabilization. J Neurosurg 1985;63:676-684 - PubMed
-
- Cybulski GR. Methods of surgical stabilization for metastatic disease of the spine. Neurosurgery 1989;25:240-252 - PubMed
-
- Persson BM, Ekelund L, Lovdahl R, Gunterberg B. Favourable results of acrylic cementation for giant cell tumors. Acta Orthop Scand 1984;55:209-214 - PubMed
-
- O' Donnell RJ, Springfield DS, Motwani HK, Ready JE, Gebhardt MC, Mankin HJ. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg 1994;76A:1827-1833 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical