

Aneurysms of the posterior cerebral artery: classification and endovascular treatment
- PMID: 11158883
- PMCID: PMC7975554
Aneurysms of the posterior cerebral artery: classification and endovascular treatment
Abstract
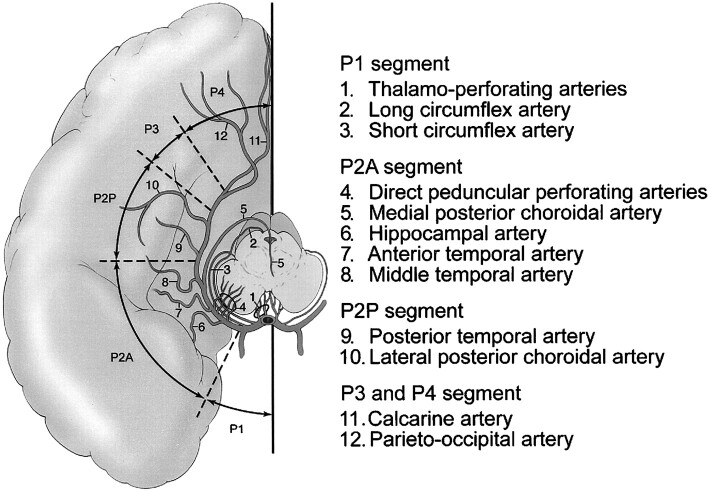
Background and purpose: We present a retrospective review of our experience in the endovascular treatment of posterior cerebral artery (PCA) aneurysms. We detail the anatomic location of these aneurysms, the technique of endovascular treatment, morphologic results, and clinical outcome. We also discuss the segmental anatomy of the PCA as it relates to the various neurologic deficits that may result from occlusion of the parent artery.
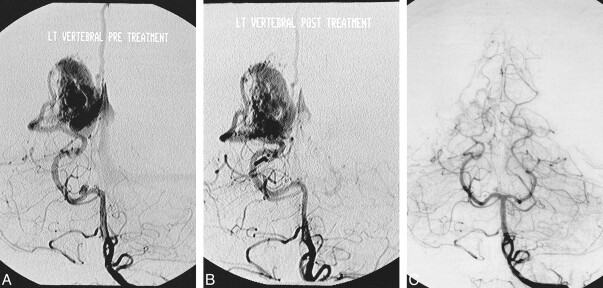
Methods: From 1993 to 1998, 20 patients (12 female, eight male; mean age, 44 yrs) harboring a PCA aneurysm were treated via an endovascular approach. One patient had two aneurysms, comprising a total of 21 lesions. Fourteen (66%) of 21 aneurysms were saccular in nature, five (24%) were giant serpentine aneurysms, and two (10%) were posttraumatic. All aneurysms were treated using Guglielmi detachable coils (GDC) either by selective obliteration of the aneurysm sac or by parent artery occlusion.
Results: Fourteen (66%) of the 21 aneurysms were successfully treated with preservation of the parent artery. In the remaining seven (33%), the parent artery was permanently occluded. The overall complication rate in this series was 15%, with a permanent morbidity rate of 10% and a 0% mortality rate.
Conclusion: Aneurysms of the PCA are rare compared with other locations in the intracranial circulation. Saccular PCA aneurysms can be treated effectively, by use of GDC, to obliterate the aneurysm yet preserve the parent artery. Fusiform and giant serpentine aneurysms of the PCA can effectively be treated by permanent occlusion of the parent artery; in these cases, thorough knowledge of the PCA segmental anatomy is crucial in order to select the site of occlusion and to avoid major neurologic deficits.
Figures

References
-
- Drake CG. Giant posterior cerebral aneurysms: 66 patients. In: Drake CG, Peerless SJ, Hruesniemi JA, eds. Surgery of Vertebrobasilar Aneurysms: London, Ontario, Experience on 1767 Patients. New York: Springer Verlag 1996;;230-248
-
- Gerber CJ, Neil-Dwyer G. A review of the management of 15 cases of aneurysms of the posterior cerebral artery. Br J Neurosurg 1992;;6:521-527 - PubMed
-
- Pia HW, Fontana H. Aneurysms of the posterior cerebral artery. Locations and clinical pictures. Acta Neurochir (Wien) 1977;;38:13-35 - PubMed
-
- Sakata S, Fujii K, Matsushima T, et al. Aneurysms of the posterior cerebral artery: report of eleven cases- surgical approaches and procedures. Neurosurgery 1993;;32:163-167 - PubMed
-
- Guglielmi G, Vinuela F, Duckwiler G, et al. Endovascular treatment of the posterior circulation aneurysms by electrothrombosis using electrically detachable coils. J Neurosurg 1992;;77:515-524 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical