

Molecular cytogenetic analysis of prostatic adenocarcinomas from screening studies : early cancers may contain aggressive genetic features
- PMID: 11159178
- PMCID: PMC1850287
- DOI: 10.1016/s0002-9440(10)63983-1
Molecular cytogenetic analysis of prostatic adenocarcinomas from screening studies : early cancers may contain aggressive genetic features
Abstract
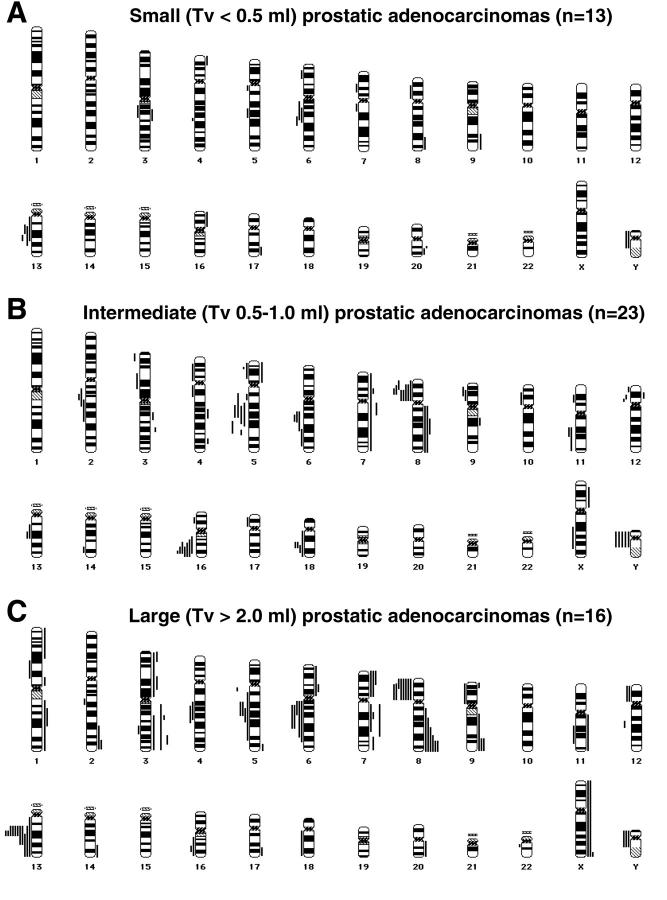
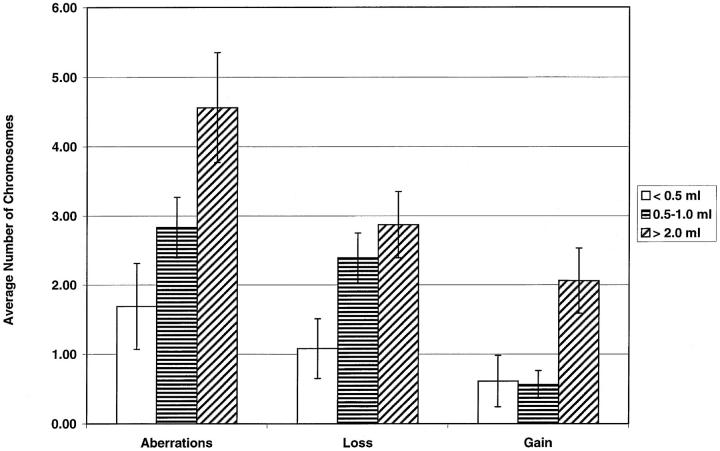
No objective parameters have been found so far that can predict the biological behavior of early stages of prostatic cancer, which are encountered frequently nowadays due to surveillance and screening programs. We have applied comparative genomic hybridization to routinely processed, paraffin-embedded radical prostatectomy specimens derived from patients who participated in the European Randomized Study of Screening for Prostate Cancer. We defined a panel consisting of 36 early cancer specimens: 13 small (total tumor volume (Tv) < 0.5 ml) carcinomas and 23 intermediate (Tv between 0.5-1.0 ml) tumors. These samples were compared with a set of 16 locally advanced, large (Tv > 2.0 ml) tumor samples, not derived from the European Randomized Study of Screening for Prostate Cancer. Chromosome arms that frequently (ie, > or = 15%) showed loss in the small tumors included 13q (31%), 6q (23%), and Y (15%), whereas frequent (ie, > or = 15%) gain was seen of 20q (15%). In the intermediate cancers, loss was detected of 8p (35%), 16q (30%), 5q (26%), Y (22%), 6q, and 18q (both 17%). No consistent gains were found in this group. In the large tumors, loss was seen of 13q (69%), 8p (50%), 5q, 6q (both 31%), and Y (15%). Gains were observed of 8q (37%), 3q (25%), 7p, 7q, 9q, and Xq (all 19%). Comparison of these early, localized tumors with large adenocarcinomas showed a significant increase in the number of aberrant chromosomes per case (Rs = 0.36, P = 0.009). The same was true for the number of lost or gained chromosomes per case (Rs = 0.27, P: = 0.05; Rs = 0.48, respectively; P < 0.001). Interestingly, chromosomal alterations that were found in previous studies to be potential biomarkers for tumor aggressiveness, ie, gain of 7pq and/or 8q, were already distinguished in the small and intermediate cancers. In conclusion, our data show that chromosomal losses, more specifically of 6q and 13q, are early events in prostatic tumorigenesis, whereas chromosomal gains, especially of 8q, appear to be late events in prostatic tumor development. Finally, early localized tumors, as detected by screening programs, harbor cancers with aggressive genetic characteristics.
Figures
References
-
- Landis SH, Murray T, Bolden S, Wingo PA: Cancer statistics, 1999. CA Cancer J Clin 1999, 4:8-31 - PubMed
-
- Stamey AT, Donaldson AN, Yemoto CE, McNeal JE, Sözen S, Gill H: Histological and clinical findings in 896 consecutive prostates treated only with radical retropubic prostatectomy: epidemiologic significance of annual changes. J Urol 1998, 160:2412-2417 - PubMed
-
- Jacobsen SJ, Katusic SK, Bergstralh EJ, Oesterling JE, Ohrt D, Klee GG, Chute CG, Lieber MM: Incidence of prostate cancer diagnosis in the eras before and after serum prostate-specific antigen testing. JAMA 1995, 274:1445-1449 - PubMed
-
- Hankey BF, Feuer EJ, Clegg LX, Hayes RB, Legler JM, Prorok PC, Ries LA, Merrill RM, Kaplan RS: Cancer surveillance series: interpreting trend in prostate cancer-part 1: Evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates. J Natl Cancer Inst 1999, 91:1017-1024 - PubMed
-
- Catalona WJ, Smith DS, Ratliff TL, Basler JW: Detection of organ-confined prostate cancer is increased through prostate-specific antigen-based screening. JAMA 1993, 270:948-954 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
