

Histopathological identification of colon cancer with microsatellite instability
- PMID: 11159189
- PMCID: PMC1850324
- DOI: 10.1016/S0002-9440(10)63994-6
Histopathological identification of colon cancer with microsatellite instability
Abstract
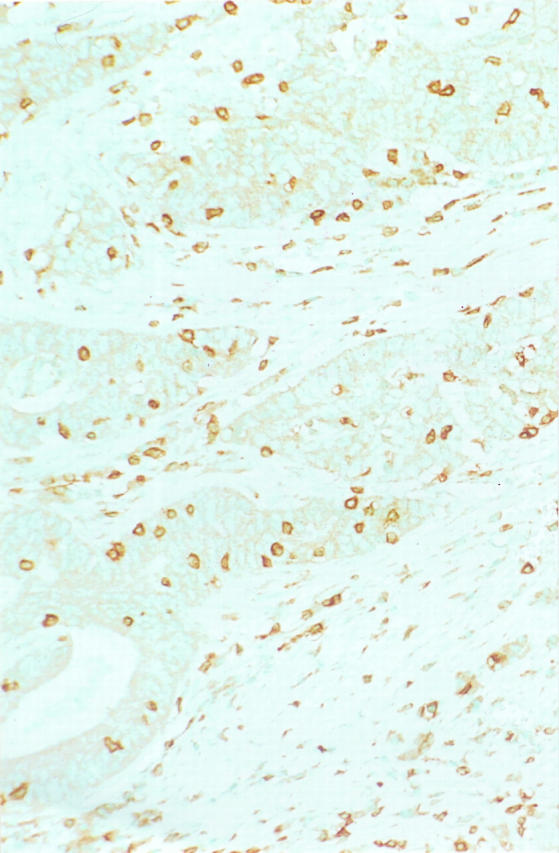
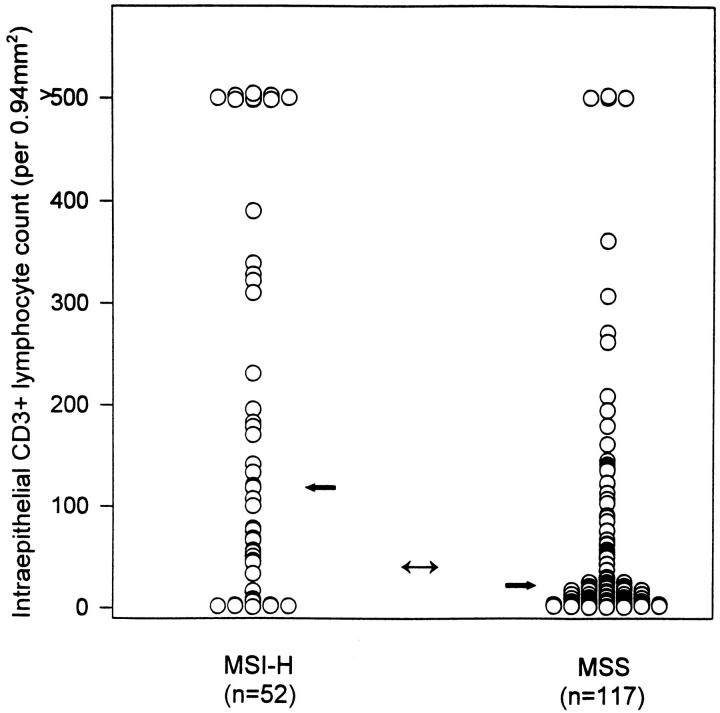
Cancer with high levels of microsatellite instability (MSI-H) is the hallmark of hereditary nonpolyposis colorectal cancer syndrome, and MSI-H occurs in approximately 15% of sporadic colorectal carcinomas that have improved prognosis. We examined the utility of histopathology for the identification of MSI-H cancers by evaluating the features of 323 sporadic carcinomas using specified criteria and comparing the results to MSI-H status. Coded hematoxylin and eosin sections were evaluated for tumor features (signet ring cells; mucinous histology; cribriforming, poor differentiation, and medullary-type pattern; sponge-like mucinous growth; pushing invasive margin) and features of host immune response (Crohn's-like lymphoid reaction, intratumoral lymphocytic infiltrate, and intraepithelial T cells by immunohistochemistry for CD3 with morphometry). Interobserver variation among five pathologists was determined. Subjective interpretation of histopathology as an indication for MSI testing was recorded. We found that medullary carcinoma, intraepithelial lymphocytosis, and poor differentiation were the best discriminators between MSI-H and microsatellite-stable cancers (odds ratio: 37.8, 9.8, and 4.0, respectively; P = 0.000003 to < 0.000001) with high specificity (99 to 87%). The sensitivities, however, were very low (14 to 38%), and interobserver agreement was good only for evaluation of poor differentiation (kappa, 0.69). Mucinous histopathological type and presence of signet ring cells had low odds ratios of 3.3 and 2.7 (P = 0.005 and P = 0.02) with specificities of 95% but sensitivities of only 15 and 13%. Subjective interpretation of the overall histopathology as suggesting MSI-H performed better than any individual feature; the odds ratio was 7.5 (P < 0.000001) with sensitivity of 49%, specificity of 89%, and moderate interobserver agreement (kappa, 0.52). Forty intraepithelial CD3-positive lymphocytes/0.94 mm2, as established by receiver operating characteristic curve analysis, resulted in an odds ratio of 6.0 (P < 0.000001) with sensitivity of 75% and specificity of 67%. Our findings indicate that histopathological evaluation can be used to prioritize sporadic colon cancers for MSI studies, but morphological prediction of MSI-H has low sensitivity, requiring molecular analysis for therapeutic decisions.
Figures


References
-
- Ionov Y, Peinado M, Malkhosyan S, Shibata D, Perucho M: Ubiquitous somatic mutations in simple repeated sequences reveal a new mechanism for colonic carcinogenesis. Nature 1993, 363:558-561 - PubMed
-
- Kolodner RD, Marsischky GT: Eukaryotic DNA mismatch repair. Curr Opin Genet Dev 1999, 9:89-96 - PubMed
-
- Aaltonen LA, Peltomaki P, Leach FS, Sistonen P, Pylkkanen L, Mecklin JP, Jarvinen H, Powell SM, Jen J, Hamilton SR, et al: Clues to the pathogenesis of familial colorectal cancer. Science 1993, 260:812-816 - PubMed
-
- Peltomaki P, Aaltonen LA, Sistonen P, Pylkkanen L, Mecklin JP, Jarvinen H, Green JS, Jass JR, Weber JL, Leach FS, et al: Genetic mapping of a locus predisposing to human colorectal cancer. Science 1993, 260:810-819 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
