

Pragmatic randomised controlled trial of two prescribing strategies for childhood acute otitis media
- PMID: 11159657
- PMCID: PMC26576
- DOI: 10.1136/bmj.322.7282.336
Pragmatic randomised controlled trial of two prescribing strategies for childhood acute otitis media
Abstract
Objective: To compare immediate with delayed prescribing of antibiotics for acute otitis media.
Design: Open randomised controlled trial.
Setting: General practices in south west England.
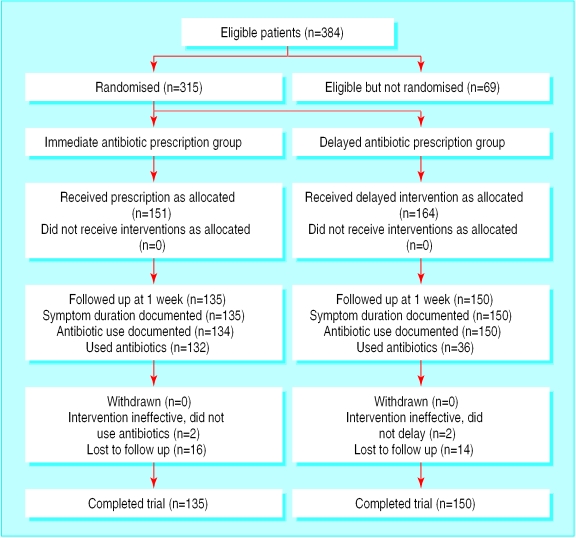
Participants: 315 children aged between 6 months and 10 years presenting with acute otitis media.
Interventions: Two treatment strategies, supported by standardised advice sheets-immediate antibiotics or delayed antibiotics (antibiotic prescription to be collected at parents' discretion after 72 hours if child still not improving).
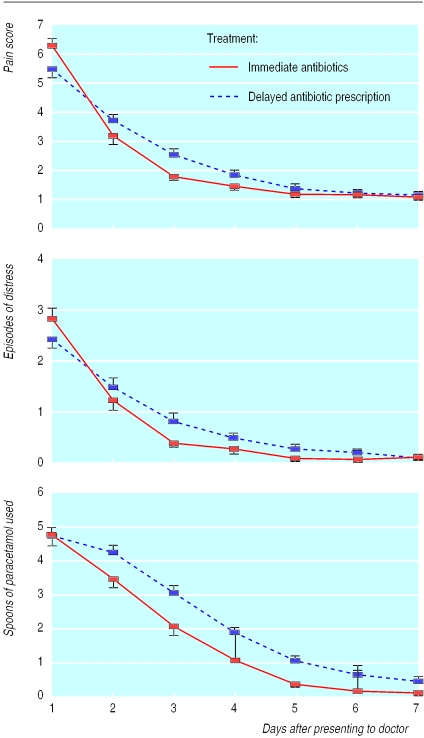
Main outcome measures: Symptom resolution, absence from school or nursery, paracetamol consumption.
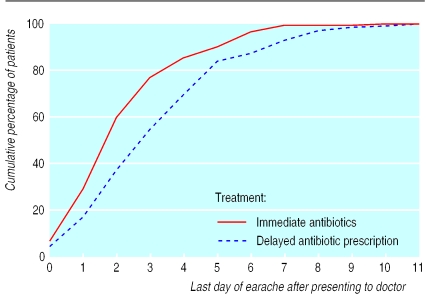
Results: On average, symptoms resolved after 3 days. Children prescribed antibiotics immediately had shorter illness (-1.1 days (95% confidence interval -0.54 to -1.48)), fewer nights disturbed (-0.72 (-0.30 to -1.13)), and slightly less paracetamol consumption (-0.52 spoons/day (-0.26 to -0.79)). There was no difference in school absence or pain or distress scores since benefits of antibiotics occurred mainly after the first 24 hours-when distress was less severe. Parents of 36/150 of the children given delayed prescriptions used antibiotics, and 77% were very satisfied. Fewer children in the delayed group had diarrhoea (14/150 (9%) v 25/135 (19%), chi(2)=5.2, P=0.02). Fewer parents in the delayed group believed in the effectiveness of antibiotics and in the need to see the doctor with future episodes.
Conclusion: Immediate antibiotic prescription provided symptomatic benefit mainly after first 24 hours, when symptoms were already resolving. For children who are not very unwell systemically, a wait and see approach seems feasible and acceptable to parents and should substantially reduce the use of antibiotics for acute otitis media.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical