

Secular trends in the epidemiology and outcome of Barrett's oesophagus in Olmsted County, Minnesota
- PMID: 11171817
- PMCID: PMC1760138
- DOI: 10.1136/gut.48.3.304
Secular trends in the epidemiology and outcome of Barrett's oesophagus in Olmsted County, Minnesota
Abstract
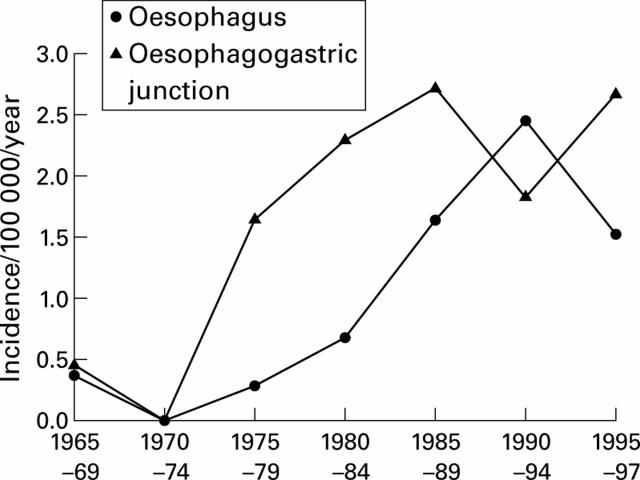
Background: The incidence of oesophageal adenocarcinoma has increased greatly. Barrett's oesophagus is a known risk factor.
Aims: To identify changes in the incidence, prevalence, and outcome of Barrett's oesophagus in a defined population.
Subjects: Residents of Olmsted County, Minnesota, with clinically diagnosed Barrett's oesophagus, or oesophageal or oesophagogastric junction adenocarcinoma.
Methods: Cases were identified using the Rochester Epidemiology Project medical records linkage system. Records were reviewed with follow up to 1 January 1998.
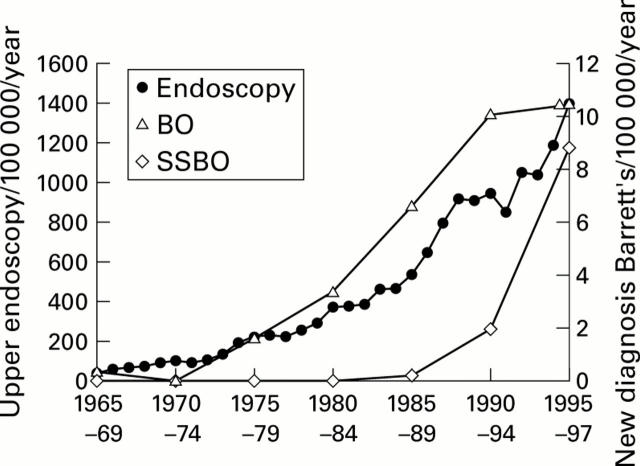
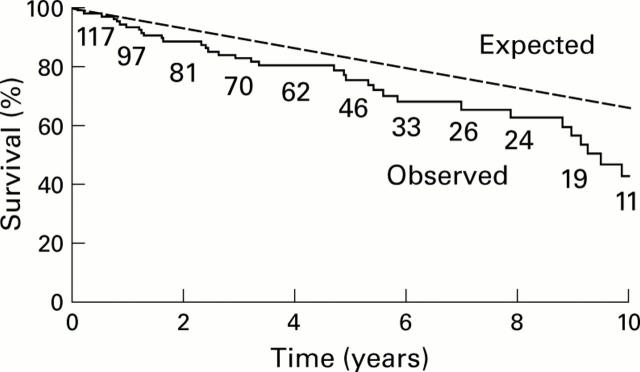
Results: The incidence of clinically diagnosed Barrett's oesophagus (>3 cm) increased 28-fold from 0.37/100 000 person years in 1965-69 to 10.5/100 000 in 1995-97. Of note, gastroscopic examinations increased 22-fold in this same time period. The prevalence of diagnosed Barrett's oesophagus increased from 22.6 (95% confidence interval (CI) 11.7-33.6) per 100 000 in 1987 to 82.6/100 000 in 1998. The prevalence of short segment Barrett's oesophagus (<3 cm) in 1998 was 33.4/ 100 000. Patients with Barrett's oesophagus had shorter than expected survival but only one patient with Barrett's oesophagus died from adenocarcinoma. Only four of 64 adenocarcinomas occurred in patients with previously known Barrett's oesophagus.
Conclusions: The incidence and prevalence of clinically diagnosed Barrett's oesophagus have increased in parallel with the increased use of endoscopy. We infer that the true population prevalence of Barrett's oesophagus has not changed greatly, although the incidence of oesophageal adenocarcinoma increased 10-fold. Many adenocarcinomas occurred in patients without a previous diagnosis of Barrett's oesophagus, suggesting that many people with this condition remain undiagnosed in the community.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical