

Endoscopic fluorescence detection of low and high grade dysplasia in Barrett's oesophagus using systemic or local 5-aminolaevulinic acid sensitisation
- PMID: 11171819
- PMCID: PMC1760120
- DOI: 10.1136/gut.48.3.314
Endoscopic fluorescence detection of low and high grade dysplasia in Barrett's oesophagus using systemic or local 5-aminolaevulinic acid sensitisation
Abstract
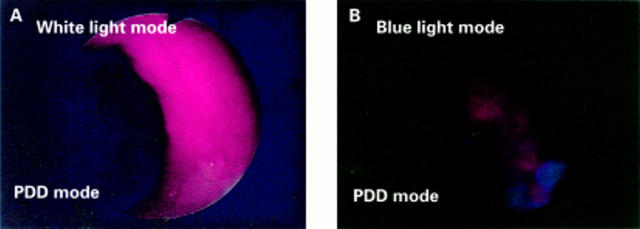
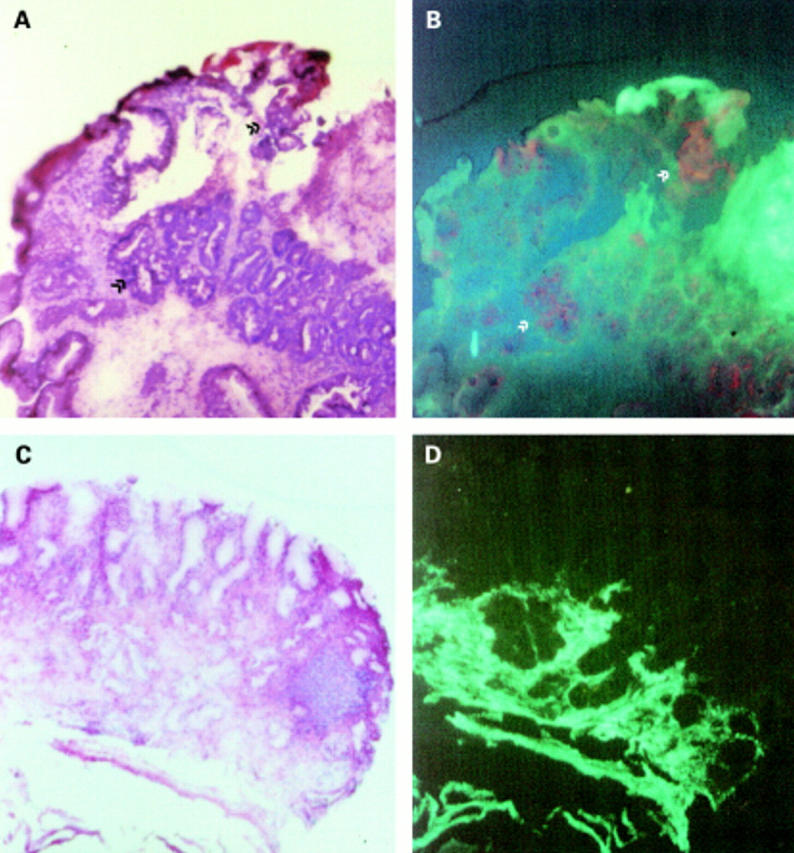
Background and aims: Barrett's oesophagus is associated with an increased risk of cancer. As dysplasia is not visible during routine endoscopy, random biopsies in the four quadrants every 1-2 cm are recommended. Endoscopic fluorescence detection (EFD) after sensitisation with 5-aminolaevulinic acid (5-ALA) with different modes and concentrations was assessed to optimise the technique for detection of dysplasia or early cancers. 5-ALA is converted intracellularly to protoporphyrin IX which accumulates in malignant tissue and can be detected by typical red fluorescence after illumination with blue light.
Methods: In 47 patients with Barrett's oesophagus, 10 with known dysplasia, 58 fluorescence endoscopies were performed after sensitisation with different concentrations of 5-ALA given orally (5, 10, 20, 30 mg/kg) or locally (500-1000 mg) by spraying the mucosa via a catheter. EFD was performed 4-6 hours after systemic and 1-2 hours after local sensitisation using a special light source delivering white or blue light. A total of 243 biopsies of red fluorescent (n=113) and non-fluorescent areas (n=130) were taken.
Results: In three patients, two early cancers and dysplasia, not visible during routine endoscopy, were detected by EFD. Thirty three biopsies revealed either low or high grade dysplasia. Sensitivity for detection of dysplastic lesions ranged from 60% after local sensitisation with 500 mg to 80%, 100%, and 100% after systemic application of 5-ALA 10, 20, and 30 mg/kg, respectively. However, specificity was best for local sensitisation (70%) while systemic administration revealed values between 27% and 56%. Using 5 mg/kg, no red fluorescence in dysplastic lesions was found. No severe side effects were noted.
Conclusion: EFD is a promising tool to detect non-visible dysplastic lesions in Barrett's oesophagus using 5-ALA sensitisation. A randomised controlled study is now indicated to compare the efficacy of EFD with the standard technique of four quadrant random biopsies.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials