

Virtual hepatic resection using three-dimensional reconstruction of helical computed tomography angioportograms
- PMID: 11176128
- PMCID: PMC1421204
- DOI: 10.1097/00000658-200102000-00011
Virtual hepatic resection using three-dimensional reconstruction of helical computed tomography angioportograms
Abstract
Objective: To establish the accuracy of virtual hepatic resection using three-dimensional (3D) models constructed from computed tomography angioportography (CTAP) images in determining the liver volume (LV) resected during resectional liver surgery.
Summary background data: The ability to measure LV before surgery could be useful in determining the extent and nature of hepatic resection. Accurate assessment of LV and an estimate of liver function may also allow prediction of postoperative liver failure in patients undergoing resection, assist in volume-enhancing embolization procedures, help with the planning of staged hepatic resection for bilobar disease, and aid in selection of living-related liver donors.
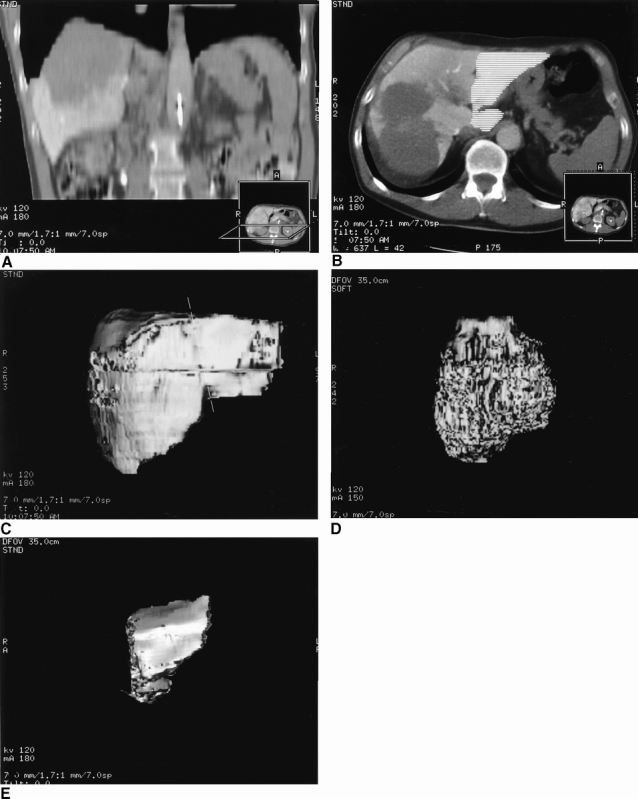
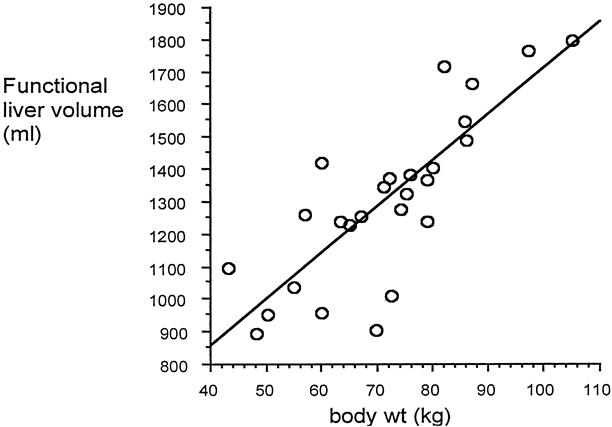
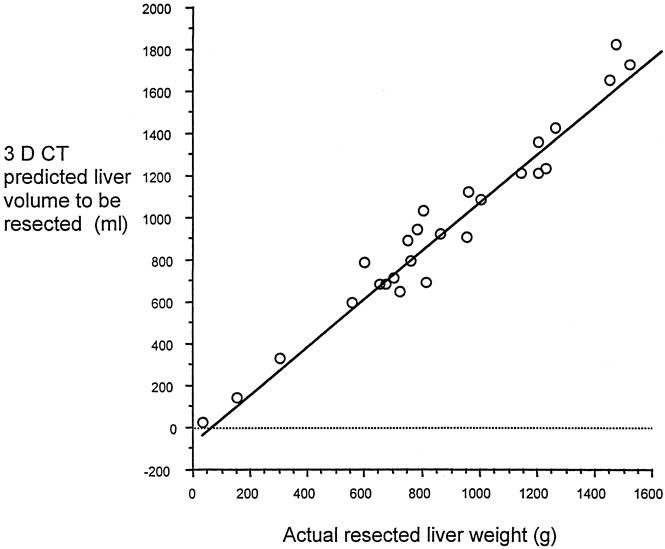
Methods: A retrospective study was conducted involving 27 patients scheduled for liver resection. Using mapping technology, 3D models were constructed from helical CTAP images. From these 3D models, tumor volume, total LV, and functional LV were calculated and were compared with body weight. The 3D liver models were subjected to a virtual hepatectomy along established anatomical planes, and the resected LV was calculated. The resected volume predicted by radiologists (unaware of the actual weight) was compared with the specimen weight measured after actual surgical resection.
Results: A significant correlation was found between body weight and functional LV but not total LV. The computer prediction of resected LV after virtual hepatectomy of 3D models compared well with resected liver weight.
Conclusion: Virtual hepatectomy of 3D CTAP reconstructed images provides an accurate prediction of liver mass removed during subsequent hepatic resection. The authors intend to combine this technology with an assessment of liver function to attempt to predict patients at risk for liver failure after hepatic resection.
Figures

References
-
- Nordlinger B, Jaeck D, Guiget M, et al. Surgical resection of hepatic metastases. Multicentric retrospective study by the French Association of Surgery. In: Nordlinger B, Jaeck D, eds. Treatment of Hepatic Metastases of Colorectal Cancer. Paris: Springer-Verlag; 1992: 1240–1246.
-
- Oellerich M, Ringe B, Gubernatis G, et al. Lignocaine metabolite formation as a measure of pre-transplant liver function. Lancet 1989; 1 (8639): 640–642. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
