

Surveillance strategies and impact of vancomycin-resistant enterococcal colonization and infection in critically ill patients
- PMID: 11176133
- PMCID: PMC1421209
- DOI: 10.1097/00000658-200102000-00016
Surveillance strategies and impact of vancomycin-resistant enterococcal colonization and infection in critically ill patients
Abstract
Objective: To determine the optimal site and frequency for vancomycin-resistant enterococci (VRE) surveillance to minimize the number of days of VRE colonization before identification and subsequent isolation.
Summary background data: The increasing prevalence of VRE and the limited therapeutic options for its treatment demand early identification of colonization to prevent transmission.
Methods: The authors conducted a 3-month prospective observational study in medical and surgical intensive care unit (ICU) patients with a stay of 3 days or more. Oropharyngeal and rectal swabs, tracheal and gastric aspirates, and urine specimens were cultured for VRE on admission to the ICU and twice weekly until discharge.
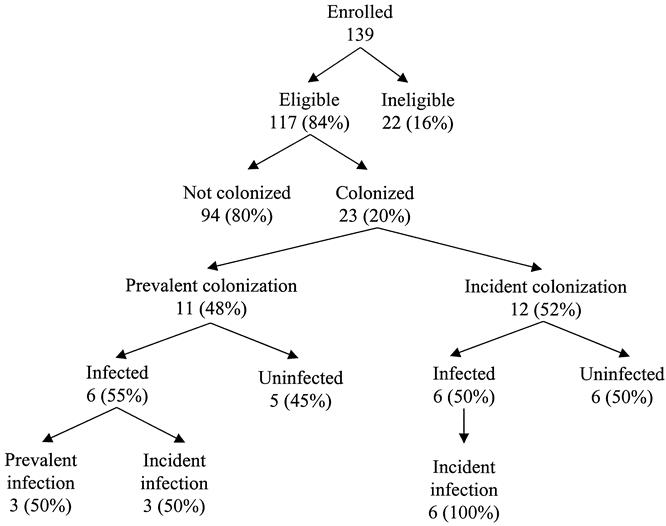
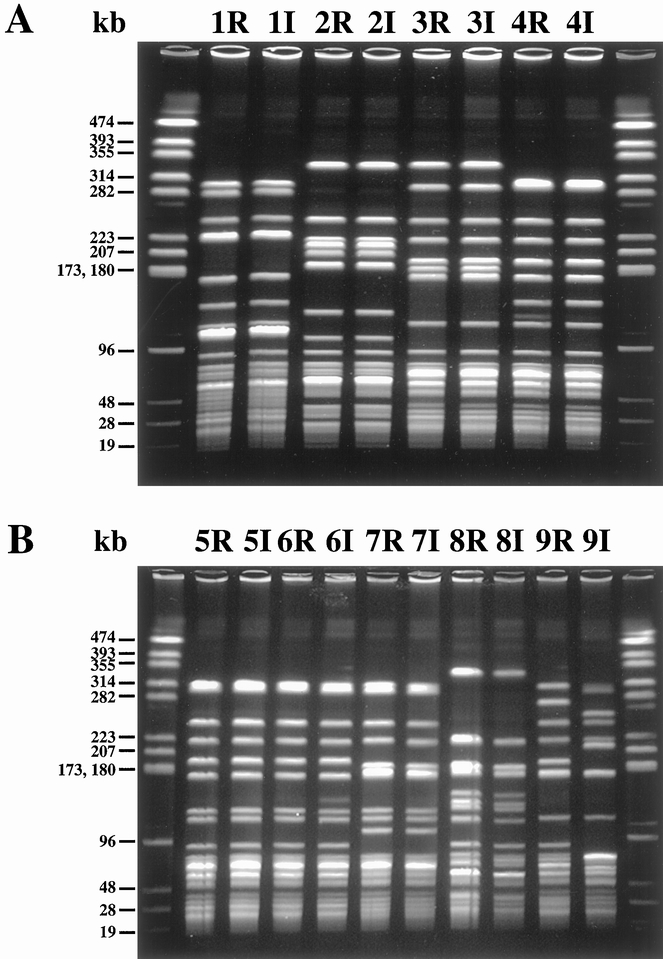
Results: Of 117 evaluable patients, 23 (20%) were colonized by VRE. Twelve patients (10%) had VRE infection. Of nine patients who developed infections after ICU admission, eight were colonized before infection. The rectum was the first site of colonization in 92% of patients, and positive rectal cultures preceded 89% of infections acquired in the ICU. This was supported by strain delineations using pulsed-field gel electrophoresis. Twice-weekly rectal surveillance alone identified 93% of the maximal estimated VRE-related patient-days; weekly or admission-only surveillance was less effective. As a test for future VRE infection, rectal surveillance culture twice weekly had a negative predictive value of 99%, a positive predictive value of 44%, and a relative risk for infection of 34.
Conclusions: Twice-weekly rectal VRE surveillance of critically ill patients is an effective strategy for early identification of colonized patients at increased risk for VRE transmission, infection, and death.
Figures
References
-
- Leclerq R, Derlot E, Duval J, Courvalin P. Plasmid-mediated resistance to vancomycin and teicoplanin in Enterococcus faecium. N Engl J Med 1988; 319: 157–161. - PubMed
-
- Schaberg DR, Culver DH, Gaynes RP. Major trends in the microbial etiology of nosocomial infections. Am J Med 1991; (suppl 3B):S72—75. - PubMed
-
- Centers for Disease Control & Prevention. Nosocomial enterococci resistant to vancomycin, United States, 1989–1993. MMWR 1993; 42: 597–599. - PubMed
-
- Mainous MR, Lipsett PA, O’Brien M. Enterococcal bacteremia in the surgical intensive care unit. Does vancomycin resistance affect mortality? The Johns Hopkins SICU Study Group. Arch Surg 1997; 132: 76–81. - PubMed
-
- Jones RN, Marshall SA, Pfaller MA, et al. Nosocomial enterococcal blood stream infections in the SCOPE Program: antimicrobial resistance, species occurrence, molecular testing results, and laboratory testing accuracy. Diagn Microbiol Infect Dis 1997; 29: 95–102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
