

Measurement of tracheal temperature is not a reliable index of total respiratory heat loss in mechanically ventilated patients
- PMID: 11178222
- PMCID: PMC29053
- DOI: 10.1186/cc974
Measurement of tracheal temperature is not a reliable index of total respiratory heat loss in mechanically ventilated patients
Abstract
Background: Minimizing total respiratory heat loss is an important goal during mechanical ventilation. The aim of the present study was to evaluate whether changes in tracheal temperature (a clinical parameter that is easy to measure) are reliable indices of total respiratory heat loss in mechanically ventilated patients.
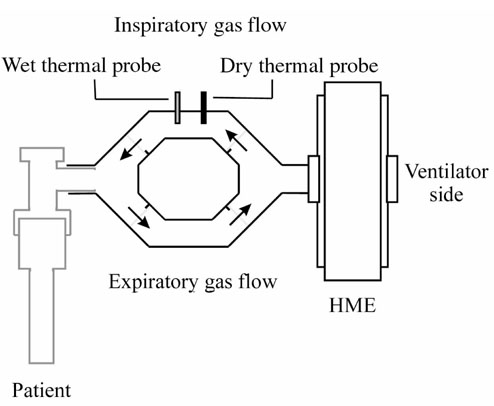
Method: Total respiratory heat loss was measured, with three different methods of inspired gas conditioning, in 10 sedated patients. The study was randomized and of a crossover design. Each patient was ventilated for three consecutive 24-h periods with a heated humidifier (HH), a hydrophobic heat-moisture exchanger (HME) and a hygroscopic HME. Total respiratory heat loss and tracheal temperature were simultaneously obtained in each patient. Measurements were obtained during each 24-h study period after 45 min, and 6 and 24 h.
Results: Total respiratory heat loss varied from 51 to 52 cal/min with the HH, from 100 to 108 cal/min with the hydrophobic HME, and from 92 to 102 cal/min with the hygroscopic HME (P < 0.01). Simultaneous measurements of maximal tracheal temperatures revealed no significant differences between the HH (35.7-35.9 degrees C) and either HME (hydrophobic 35.3-35.4 degrees C, hygroscopic 36.2-36.3 degrees C).
Conclusion: In intensive care unit (ICU) mechanically ventilated patients, total respiratory heat loss was twice as much with either hydrophobic or hydroscopic HME than with the HH. This suggests that a much greater amount of heat was extracted from the respiratory tract by the HMEs than by the HH. Tracheal temperature, although simple to measure in ICU patients, does not appear to be a reliable estimate of total respiratory heat loss.
Figures
Comment in
-
The upper airway--the forgotten organ.Crit Care. 2001;5(1):1-2. doi: 10.1186/cc971. Epub 2001 Jan 9. Crit Care. 2001. PMID: 11178219 Free PMC article.
Similar articles
-
Comparing two heat and moisture exchangers with one vaporizing humidifier in patients with minute ventilation greater than 10 L/min.Chest. 1995 May;107(5):1411-5. doi: 10.1378/chest.107.5.1411. Chest. 1995. PMID: 7750340 Clinical Trial.
-
Changing a hydrophobic heat and moisture exchanger after 48 hours rather than 24 hours: a clinical and microbiological evaluation.Intensive Care Med. 1999 Nov;25(11):1237-43. doi: 10.1007/s001340051051. Intensive Care Med. 1999. PMID: 10654207
-
[Air conditioning with a high-performance HME (heat and moisture exchanger)--an effective and economical alternative to active humidifiers in ventilated patients. A prospective and randomized clinical study].Anaesthesist. 1996 Jun;45(6):518-25. doi: 10.1007/s001010050285. Anaesthesist. 1996. PMID: 8767565 Clinical Trial. German.
-
Heated humidification versus heat and moisture exchangers for ventilated adults and children.Anesth Analg. 2010 Oct;111(4):1072. doi: 10.1213/ANE.0b013e3181efb538. Anesth Analg. 2010. PMID: 20870984 Review.
-
Devices used to humidify respired gases.Respir Care Clin N Am. 2006 Jun;12(2):165-82. doi: 10.1016/j.rcc.2006.03.012. Respir Care Clin N Am. 2006. PMID: 16828689 Review.
Cited by
-
Airway humidification with a heat and moisture exchanger in mechanically ventilated neonates : a preliminary evaluation.Intensive Care Med. 2007 Feb;33(2):336-43. doi: 10.1007/s00134-006-0466-1. Epub 2006 Dec 13. Intensive Care Med. 2007. PMID: 17165022 Clinical Trial.
-
Comparison of core temperature using tracheal thermometer and pulmonary artery catheter in adult patients undergoing coronary artery bypass graft surgery.PLoS One. 2025 Jan 2;20(1):e0314322. doi: 10.1371/journal.pone.0314322. eCollection 2025. PLoS One. 2025. PMID: 39746099 Free PMC article.
-
Comparison of tracheal versus esophageal temperatures during laparoscopic surgery.Can J Anaesth. 2024 May;71(5):619-628. doi: 10.1007/s12630-024-02721-5. Epub 2024 Mar 11. Can J Anaesth. 2024. PMID: 38468077 English.
-
Heat and moisture exchangers (HMEs) and heated humidifiers (HHs) in adult critically ill patients: a systematic review, meta-analysis and meta-regression of randomized controlled trials.Crit Care. 2017 May 29;21(1):123. doi: 10.1186/s13054-017-1710-5. Crit Care. 2017. PMID: 28552074 Free PMC article.
-
Heat and moisture exchangers versus heated humidifiers for mechanically ventilated adults and children.Cochrane Database Syst Rev. 2017 Sep 14;9(9):CD004711. doi: 10.1002/14651858.CD004711.pub3. Cochrane Database Syst Rev. 2017. PMID: 28905374 Free PMC article.
References
-
- Chalon J, Loew D, Malebranche J. Effect of dry anesthetic gases on tracheobronchial ciliated epithelium. Anesthesiology. 1972;37:338–343. - PubMed
-
- Stone DR, Downs JB, Paul WL, Perkins HM. Adult body temperature and heated humidification of anesthetic gases during general anesthesia. Anesth Analg. 1981;60:736–741. - PubMed
-
- Hedley RM, Allt-Graham J. Heat and moisture exchangers and breathing filters. Br J Anaesth. 1994;73:227–236. - PubMed
-
- Chalon J, Patel C, Ali M, Turndorf H, Fischgrund GK. Humidity and the anesthetized patient. Anesthesiology. 1979;50:195–198. - PubMed
-
- Forbes AR. Humidification and mucus flow in the intubated trachea. Br J Anaesth. 1973;45:874–878. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
