

Performance of the score systems Acute Physiology and Chronic Health Evaluation II and III at an interdisciplinary intensive care unit, after customization
- PMID: 11178223
- PMCID: PMC29054
- DOI: 10.1186/cc975
Performance of the score systems Acute Physiology and Chronic Health Evaluation II and III at an interdisciplinary intensive care unit, after customization
Abstract
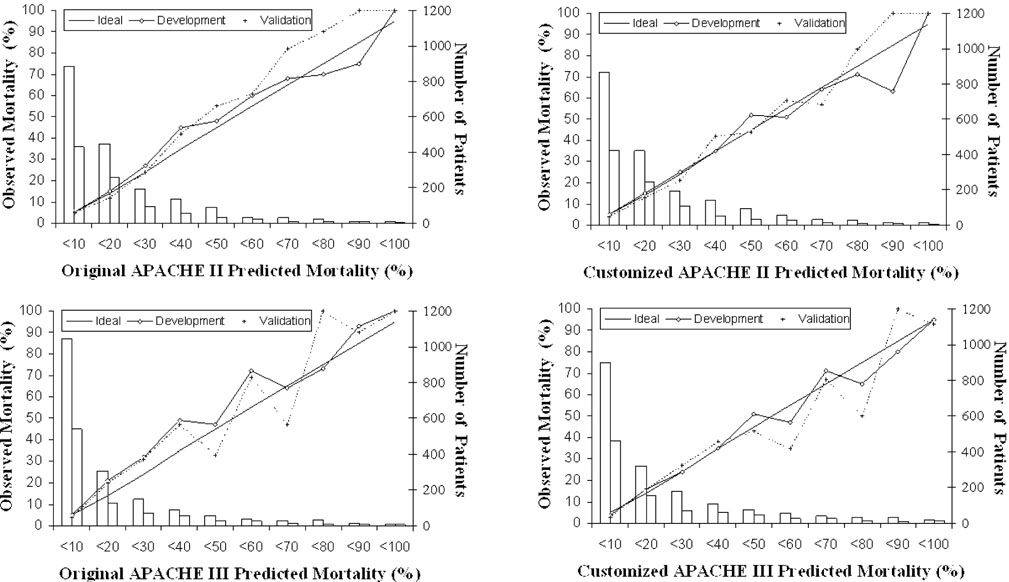
Background: Mortality predictions calculated using scoring scales are often not accurate in populations other than those in which the scales were developed because of differences in case-mix. The present study investigates the effect of first-level customization, using a logistic regression technique, on discrimination and calibration of the Acute Physiology and Chronic Health Evaluation (APACHE) II and III scales.
Method: Probabilities of hospital death for patients were estimated by applying APACHE II and III and comparing these with observed outcomes. Using the split sample technique, a customized model to predict outcome was developed by logistic regression. The overall goodness-of-fit of the original and the customized models was assessed.
Results: Of 3383 consecutive intensive care unit (ICU) admissions over 3 years, 2795 patients could be analyzed, and were split randomly into development and validation samples. The discriminative powers of APACHE II and III were unchanged by customization (areas under the receiver operating characteristic [ROC] curve 0.82 and 0.85, respectively). Hosmer-Lemeshow goodness-of-fit tests showed good calibration for APACHE II, but insufficient calibration for APACHE III. Customization improved calibration for both models, with a good fit for APACHE III as well. However, fit was different for various subgroups.
Conclusions: The overall goodness-of-fit of APACHE III mortality prediction was improved significantly by customization, but uniformity of fit in different subgroups was not achieved. Therefore, application of the customized model provides no advantage, because differences in case-mix still limit comparisons of quality of care.
Figures
Similar articles
-
Prediction of outcome from intensive care: a prospective cohort study comparing Acute Physiology and Chronic Health Evaluation II and III prognostic systems in a United Kingdom intensive care unit.Crit Care Med. 1997 Jan;25(1):9-15. doi: 10.1097/00003246-199701000-00006. Crit Care Med. 1997. PMID: 8989170
-
Prediction of outcome in intensive care unit trauma patients: a multicenter study of Acute Physiology and Chronic Health Evaluation (APACHE), Trauma and Injury Severity Score (TRISS), and a 24-hour intensive care unit (ICU) point system.J Trauma. 1999 Aug;47(2):324-9. doi: 10.1097/00005373-199908000-00017. J Trauma. 1999. PMID: 10452468
-
Should the pre-sedation Glasgow Coma Scale value be used when calculating Acute Physiology and Chronic Health Evaluation scores for sedated patients? Scottish Intensive Care Society Audit Group.Crit Care Med. 2000 Feb;28(2):389-94. doi: 10.1097/00003246-200002000-00017. Crit Care Med. 2000. PMID: 10708172 Clinical Trial.
-
Predicting outcome in critical care: the current status of the APACHE prognostic scoring system.Can J Anaesth. 1991 Apr;38(3):374-83. doi: 10.1007/BF03007629. Can J Anaesth. 1991. PMID: 2036699 Review.
-
[Scoring systems in intensive care medicine : principles, models, application and limits].Anaesthesist. 2011 Oct;60(10):963-74. doi: 10.1007/s00101-011-1942-8. Anaesthesist. 2011. PMID: 21997474 Review. German.
Cited by
-
Prevalence of deep vein thrombosis in acutely admitted ambulatory non-surgical intensive care unit patients.BMC Res Notes. 2014 Jul 5;7:431. doi: 10.1186/1756-0500-7-431. BMC Res Notes. 2014. PMID: 24996222 Free PMC article.
-
Model for End-stage Liver Disease excluding INR (MELD-XI) score in critically ill patients: Easily available and of prognostic relevance.PLoS One. 2017 Feb 2;12(2):e0170987. doi: 10.1371/journal.pone.0170987. eCollection 2017. PLoS One. 2017. PMID: 28151948 Free PMC article.
-
APACHE III outcome prediction in patients admitted to the intensive care unit after liver transplantation: a retrospective cohort study.BMC Surg. 2009 Jul 29;9:11. doi: 10.1186/1471-2482-9-11. BMC Surg. 2009. PMID: 19640303 Free PMC article.
-
Predictive value of outcome scores in patients suffering from cardiogenic shock complicating AMI: APACHE II, APACHE III, Elebute-Stoner, SOFA, and SAPS II.Med Klin Intensivmed Notfmed. 2013 Nov;108(8):666-74. doi: 10.1007/s00063-013-0234-2. Epub 2013 Apr 6. Med Klin Intensivmed Notfmed. 2013. PMID: 23558639
-
Incidence and long-term outcomes of adult patients with diabetic ketoacidosis admitted to intensive care: A retrospective cohort study.J Intensive Care Soc. 2016 Aug;17(3):222-233. doi: 10.1177/1751143716644458. Epub 2016 Apr 25. J Intensive Care Soc. 2016. PMID: 28979495 Free PMC article.
References
-
- Bodmann KF, Ehlers B, Häbel U, Ritschel P, Rühmkorf K. Epidemiologic and prognostic data of 2054 patients in a medical intensive care unit. Dtsch Med Wochenschr. 1997;122:919–925. - PubMed
-
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. An evaluation of outcome from intensive care in major medical centers. Ann Intern Med. 1986;104:410–418. - PubMed
-
- Shortell SM, Zimmerman JE, Rousseau DM, Gillies RR, Wagner DP, Draper EA, Knaus WA, Duffy J. The performance of intensive care units: does good management make a difference? Med Care. 1994;32:508–525. - PubMed
-
- Beck DH, Taylor BL, Millar B, Smith GB. Prediction of outcome from intensive care: a prospective cohort study comparing Acute Physiology and Chronic Health Evaluation II and III prognostic systems in a United Kingdom intensive care unit. Crit Care Med. 1997;25:9–15. - PubMed
-
- Moreno R, Miranda DR, Fidler V, Van Schilfgaarde R. Evaluation of two outcome prediction models on an independent database. Crit Care Med. 1998;26:50–61. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
