

Aspirin for primary prevention of coronary heart disease: safety and absolute benefit related to coronary risk derived from meta-analysis of randomised trials
- PMID: 11179262
- PMCID: PMC1729640
- DOI: 10.1136/heart.85.3.265
Aspirin for primary prevention of coronary heart disease: safety and absolute benefit related to coronary risk derived from meta-analysis of randomised trials
Abstract
Objective: To determine the cardiovascular and coronary risk thresholds at which aspirin for primary prevention of coronary heart disease is safe and worthwhile.
Design: Meta-analysis of four randomised controlled trials of aspirin for primary prevention. The benefit and harm from aspirin treatment were examined to determine: (1) the cardiovascular and coronary risk threshold at which benefit in prevention of myocardial infarction exceeds harm from significant bleeding; and (2) the absolute benefit expressed as number needed to treat (NNT) for aspirin net of cerebral haemorrhage and other bleeding complications at different levels of coronary risk.
Main outcome measures: Benefit from aspirin, expressed as reduction in cardiovascular events, myocardial infarctions, strokes, and total mortality; harm caused by aspirin in relation to significant bleeds and major haemorrhages.
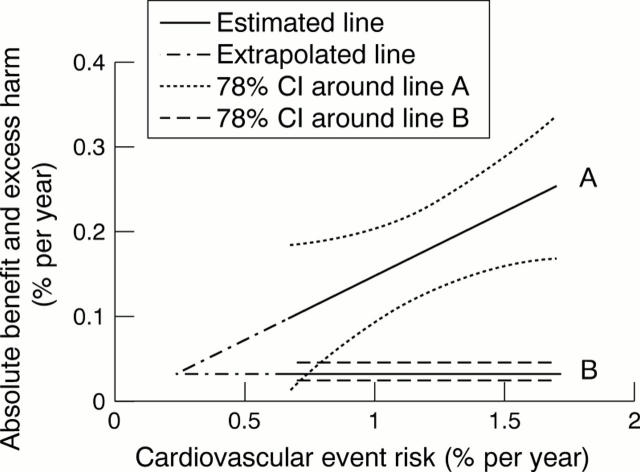
Results: Aspirin for primary prevention significantly reduced all cardiovascular events by 15% (95% confidence interval (CI) 6% to 22%) and myocardial infarctions by 30% (95% CI 21% to 38%), and non-significantly reduced all deaths by 6% (95% CI -4% to 15%). Aspirin non-significantly increased strokes by 6% (95% CI -24% to 9%) and significantly increased bleeding complications by 69% (95% CI 38% to 107%). The risk of major bleeding balanced the reduction in cardiovascular events when cardiovascular event risk was 0.22%/year. The upper 95% CI for this estimate suggests that harm from aspirin is unlikely to outweigh benefit provided the cardiovascular event risk is 0.8%/year, equivalent to a coronary risk of 0.6%/year. At coronary event risk 1.5%/year, the five year NNT was 44 to prevent a myocardial infarction, and 77 to prevent a myocardial infarction net of any important bleeding complication. At coronary event risk 1%/year the NNT was 67 to prevent a myocardial infarction, and 182 to prevent a myocardial infarction net of important bleeding.
Conclusions: Aspirin treatment for primary prevention is safe and worthwhile at coronary event risk >/= 1.5%/year; safe but of limited value at coronary risk 1%/year; and unsafe at coronary event risk 0.5%/year. Advice on aspirin for primary prevention requires formal accurate estimation of absolute coronary event risk.
Figures
Comment in
-
Who should take aspirin for primary prophylaxis of coronary heart disease?Heart. 2001 Mar;85(3):245-6. doi: 10.1136/heart.85.3.245. Heart. 2001. PMID: 11179252 Free PMC article. No abstract available.
-
Polypill. Faulty logic justifies aspirin use for primary prevention of cardiovascular disease.BMJ. 2013 Aug 9;347:f5021. doi: 10.1136/bmj.f5021. BMJ. 2013. PMID: 23935087 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical