

Impact of tuberculosis (TB) on HIV-1 activity in dually infected patients
- PMID: 11207653
- PMCID: PMC1905977
- DOI: 10.1046/j.1365-2249.2001.01401.x
Impact of tuberculosis (TB) on HIV-1 activity in dually infected patients
Abstract
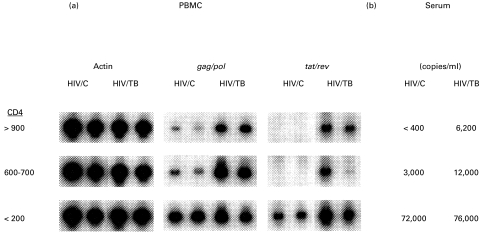
Active TB in HIV-1-infected subjects is associated with increased HIV-1-related immunodeficiency and mortality. We assessed plasma viral load in HIV-1-infected patients with pulmonary TB (HIV/TB) and non-TB symptomatic HIV-1-infected patients (HIV). HIV-1 load was higher in HIV/TB compared with HIV at higher CD4 counts (> 500/microl) (P < 0.01), but not at lower CD4 counts (< 500/microl). We also evaluated the status of HIV-1 gene expression in peripheral blood mononuclear cells (PBMC) and serum from HIV/TB and CD4-matched healthy HIV-infected patients (HIV/C) by reverse transcriptase-polymerase chain reaction over a range of CD4 (> 900/microl to < 200/microl). HIV-1 RNA in serum and PBMC correlated to one another, and both were markedly higher in HIV/TB compared with HIV/C with higher CD4 counts. Also, during a longitudinal study of anti-tuberculous chemoprophylaxis in HIV-1-infected patients, 10 subjects who developed TB had serologies before, at the time, and after the diagnosis of TB. These HIV/TB patients had an increase in viral load (average 2.5-fold) at the time of diagnosis of TB (P < 0.05). Overall, these data indicate that the transcriptional activity of HIV-1 is enhanced in HIV-1-infected patients with active TB, especially during early HIV-1 disease. As TB often is an early HIV-1 opportunistic infection, it may particularly favour early viral replication and dissemination, and therefore contribute to progression of HIV-1 disease.
Figures



References
-
- Dye C, Scheele S, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA. 1999;282:677–86. - PubMed
-
- Kumar S. WHO gives southeast Asia a health warning. Lancet. 1999;354:1010–1. - PubMed
-
- Lucas S, Nelson AM. Tuberculosis: pathogenesis, protection, and control. Washington, DC: ASM Press; 1994. Pathogenesis of tuberculosis in human immunodeficiency virus-infected people; pp. 503–13.
-
- Whalen C, Horsburgh CR, Hom D, Lahart C, Simberkoff M, Ellner J. Accelerated course of human immunodeficiency virus infection after tuberculosis. Am J Respir Crit Care Med. 1995;151:129–35. - PubMed
-
- Orenstein JM, Fox C, Wahl SM. Macrophages as a source of HIV during opportunistic infections. Science. 1997;276:1857–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
