

Value of nasal endoscopy and probing in the diagnosis and management of children with congenital epiphora
- PMID: 11222337
- PMCID: PMC1723899
- DOI: 10.1136/bjo.85.3.314
Value of nasal endoscopy and probing in the diagnosis and management of children with congenital epiphora
Abstract
Background: Congenital nasolacrimal obstruction is usually the result of failure of canalisation of the distal end of the nasolacrimal duct. The most common outcome is spontaneous resolution, but some children do require surgical treatment by probing. Probing is a blind procedure with a recognised failure rate.
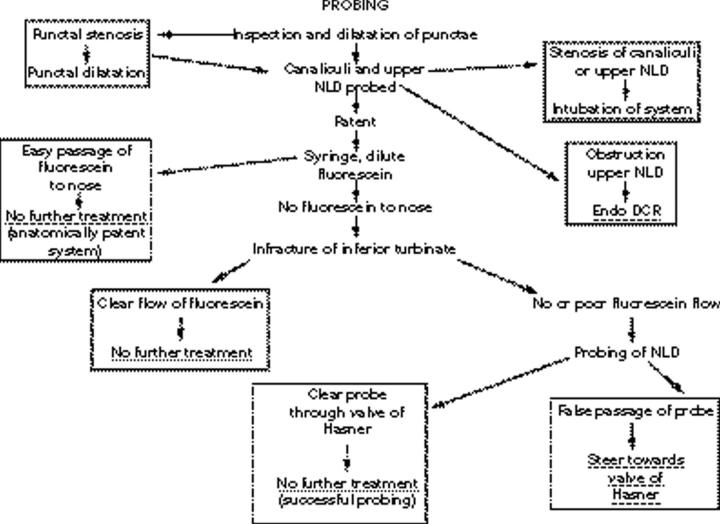
Methods: In 52 lacrimal systems of 40 children nasal endoscopy was combined with a "stepwise" systematic probing in an attempt to improve the outcome and reduce the number of repeat procedures.
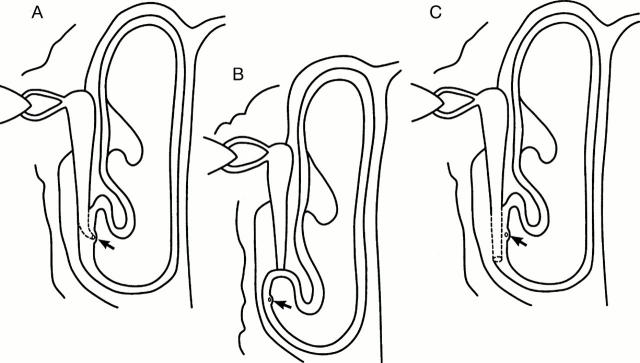
Results: Combined nasal endoscopy and probing improved the understanding of outflow obstruction in young children. The success of the procedure depended upon the level of the obstruction within the outflow system. Formation of a false passage was seen in six cases (15%). The probe was rerouted under direct visualisation in these cases to form a functioning passage. Reasons for failure were identified in those who did not have a successful outcome and only one repeat procedure was required.
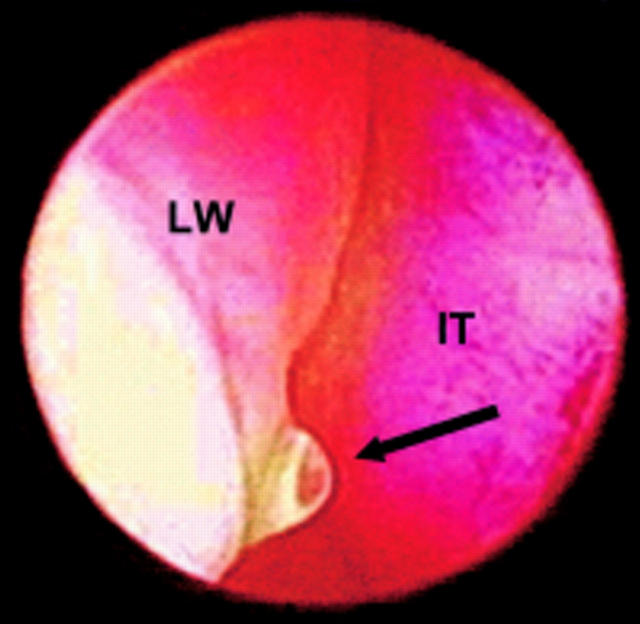
Conclusion: Using nasal endoscopy the area of lacrimal outflow obstruction at the lower end of the nasolacrimal duct can be observed directly and it is possible to guide the progress of probing under direct vision. This gives better information about the nature of the obstruction, minimises the formation of false passages, and allows a wider range of treatment options under a single anaesthetic.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical