

Selection criteria for hepatectomy in patients with hepatocellular carcinoma and portal vein tumor thrombus
- PMID: 11224626
- PMCID: PMC1421254
- DOI: 10.1097/00000658-200103000-00012
Selection criteria for hepatectomy in patients with hepatocellular carcinoma and portal vein tumor thrombus
Abstract
Objective: To examine the usefulness of the authors' method involving preoperative transcatheter arterial chemoembolization followed by hepatectomy.
Summary background data: The presence of portal vein tumor thrombus in a patient with hepatocellular carcinoma is one of the most significant factors for a poor prognosis. No standard therapy has been established.
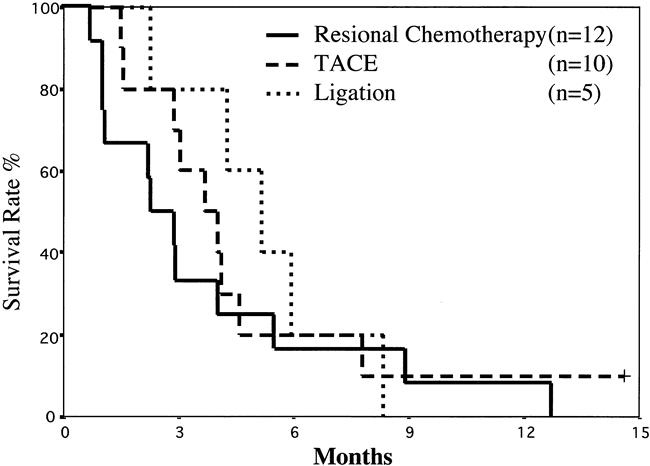
Methods: Forty-five of 455 patients with hepatocellular carcinoma (10%) from 1989 to 1998 were included in this study. These patients had gross portal vein tumor thrombus but no distant metastases. The 23 patients (50%) who had indications for surgery received preoperative transcatheter arterial chemoembolization: 18 underwent hepatic resection and 5 underwent ligation of the hepatic artery or portal vein on laparotomy. Among the remaining 22 patients who did not have indications for hepatectomy, 10 received regional chemotherapy and 12 underwent transcatheter arterial chemoembolization.
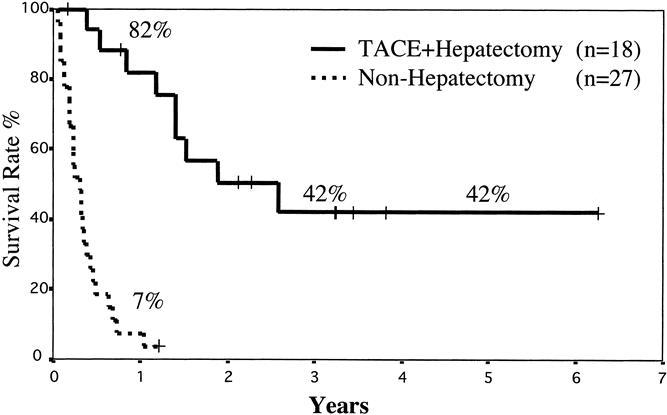
Results: The mean duration of survival was 3.4 +/- 2.7 years in the 18 patients who received transcatheter arterial chemoembolization and hepatectomy and 0.36 +/- 0.26 years in the 27 patients who did not receive hepatectomy. The survival rate of the 18 patients who received hepatic resection with preoperative transcatheter arterial chemoembolization was 82% at 1 year, 42% at 3 years, and 42% at 5 years. Portal trunk occlusion by tumor thrombus, three or more primary nodules, an indocyanine green retention rate at 15 minutes of 20% or worse, and therapeutic choice other than hepatectomy were significant predictors of a poor prognosis on univariate analysis. Hepatectomy was the only factor that was significant on multivariate analysis.
Conclusions: Patients may enjoy long-term survival if they receive hepatectomy with preoperative transcatheter arterial chemoembolization, when the number of primary nodules is no more than two, the portal trunk is not occluded by tumor thrombus, and the indocyanine green retention rate at 15 minutes is better than 20%.
Figures
References
-
- Stuart KE, Anand AJ, Jenkins RL. Hepatocellular carcinoma in the United States. Prognostic features, treatment outcome, and survival. Cancer 1996; 77: 2217–2222. - PubMed
-
- Llovet JM, Bustamante J, Castells A, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology 1999; 29: 62–67. - PubMed
-
- Okada S, Okazaki N, Nose H, et al. Prognostic factors in patients with hepatocellular carcinoma receiving systemic chemotherapy. Hepatology 1992; 16: 112–117. - PubMed
-
- Ando E, Yamashita F, Tanaka M, et al. A novel chemotherapy for advanced hepatocellular carcinoma with tumor thrombosis of the main trunk of the portal vein. Cancer 1997; 79: 1890–1896. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
