

Impact of increasing comorbidity on infrainguinal reconstruction: a 20-year perspective
- PMID: 11224635
- PMCID: PMC1421261
- DOI: 10.1097/00000658-200103000-00021
Impact of increasing comorbidity on infrainguinal reconstruction: a 20-year perspective
Abstract
Objective: To examine trends in patient and procedural variables and outcomes associated with autogenous lower extremity arterial reconstruction (LER) in a single center during a period of two decades.
Summary background data: Surgical arterial reconstruction is of proven value in the therapy of patients with critical ischemia of the lower extremities. Changing demographics and increasing comorbidity are resulting in an increasing prevalence and associated complexity of peripheral vascular disease. The effect of these variables on the types and outcomes of surgical reconstructions is not known.
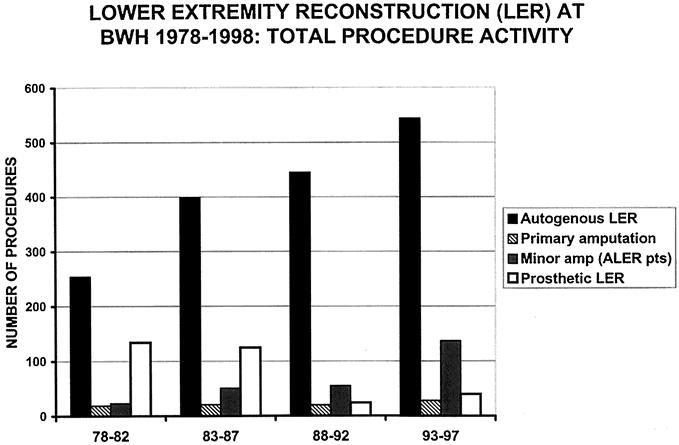
Methods: The authors performed a retrospective analysis of all autogenous LER procedures performed at their institution from 1978 to 1997. Procedures were divided into 5-year intervals: group 1, 1978 to 1982; group 2, 1983 to 1987; group 3, 1988 to 1992; group 4, 1993 to 1997. Categorical parameters were compared using chi-square analysis; rates were computed by the life-table method and compared using Mantel-Cox log-rank analysis.
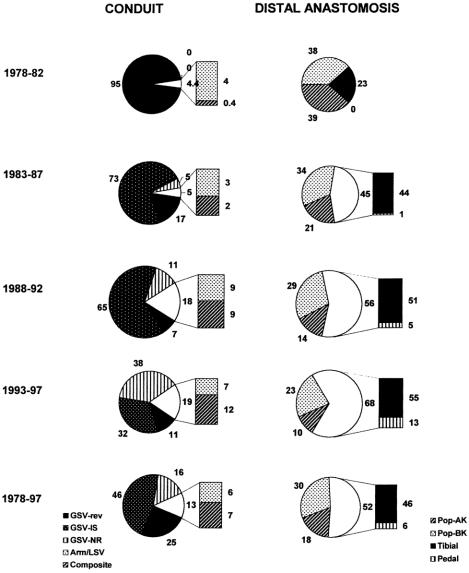
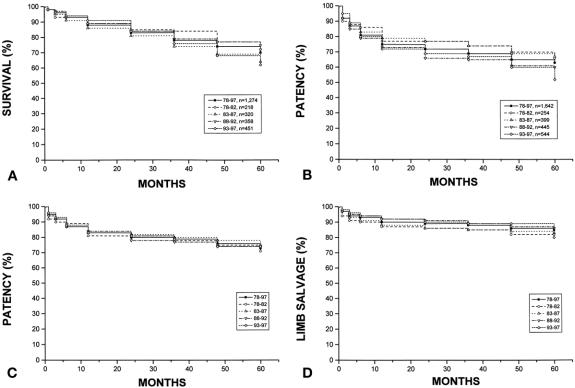
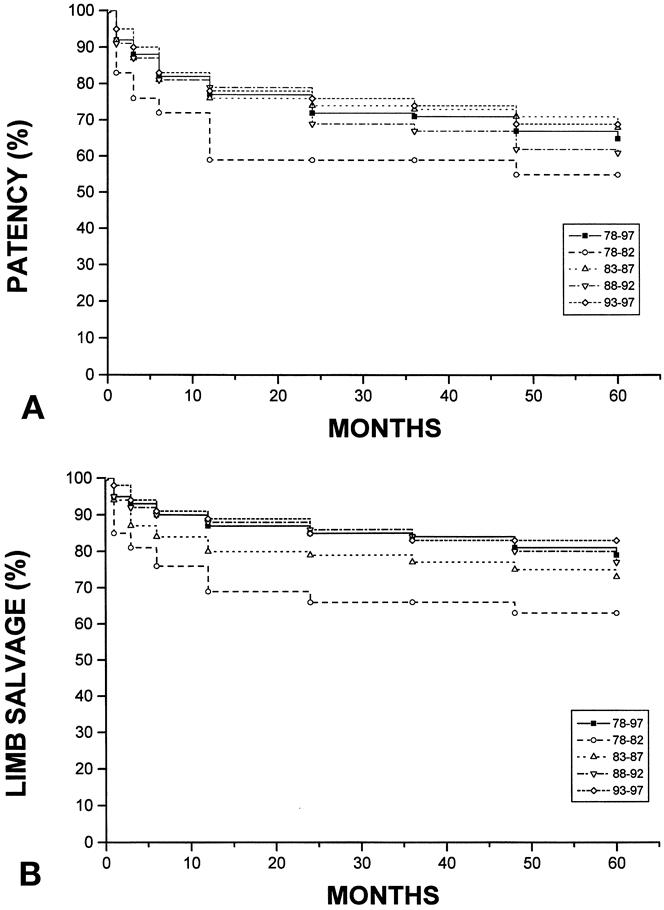
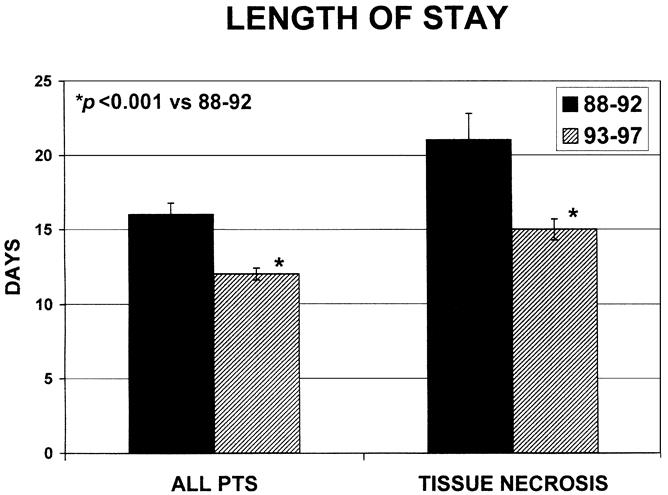
Results: A total of 1,642 autogenous LER procedures were performed in 1,274 patients. A significant increase in age, female gender, diabetes mellitus, renal failure, and prior coronary artery bypass grafting was noted in group 4. Increased technical complexity in this group was reflected by a greater incidence of tissue necrosis as the indication for LER, the use of ectopic or composite vein, and more distal levels of outflow. The surgical death rate remained unchanged (2%) throughout. Patient survival, primary and secondary graft patency, and limb salvage at 5 years for the entire cohort were 70 +/- 2%, 63 +/- 2%, 73 +/- 1%, and 85 +/- 1%, respectively. Hospital length of stay was reduced 25% from a mean of 15.7 +/- 0.8 days in group 3 to 11.7 +/- 0.4 days in group 4.
Conclusion: In a tertiary practice setting, patients requiring LER present an increasingly complex medical and surgical challenge compared with the previous decade. Excellent outcomes may still be achieved by an aggressive approach relying on autogenous vein conduit.
Figures
References
-
- U. S. Bureau of the Census. Statistical Abstract of the United States: 1993. 113th ed. Washington, DC: U.S. Government Printing Office; 1993:91.
-
- Taylor LM Jr, Edwards JM, Porter JM. Present status of reversed vein bypass grafting: five-year results of a modern series. J Vasc Surg 1990; 11: 193–206. - PubMed
-
- Belkin M, Conte MS, Donaldson MC, et al. The impact of gender on the results of arterial bypass with in-situ greater saphenous vein. Am J Surg 1995; 170: 97–102. - PubMed
-
- Kent KC, Whittemore AD, Mannick JA. Short-term and midterm results of an all-autogenous tissue policy for infrainguinal reconstruction. J Vasc Surg 1989; 9: 107–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
