

JC virus-specific cytotoxic T lymphocytes in individuals with progressive multifocal leukoencephalopathy
- PMID: 11238876
- PMCID: PMC114143
- DOI: 10.1128/JVI.75.7.3483-3487.2001
JC virus-specific cytotoxic T lymphocytes in individuals with progressive multifocal leukoencephalopathy
Abstract
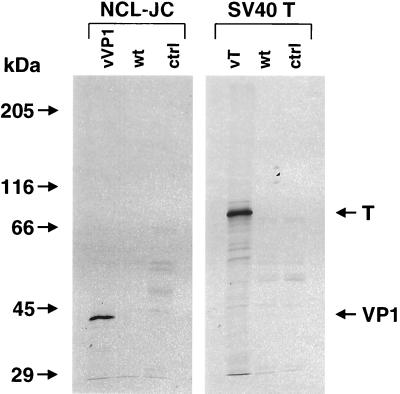
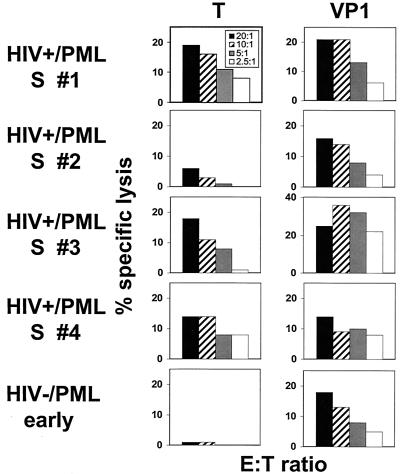
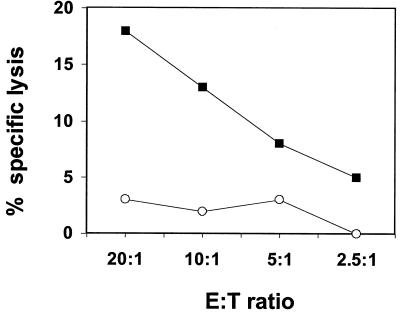
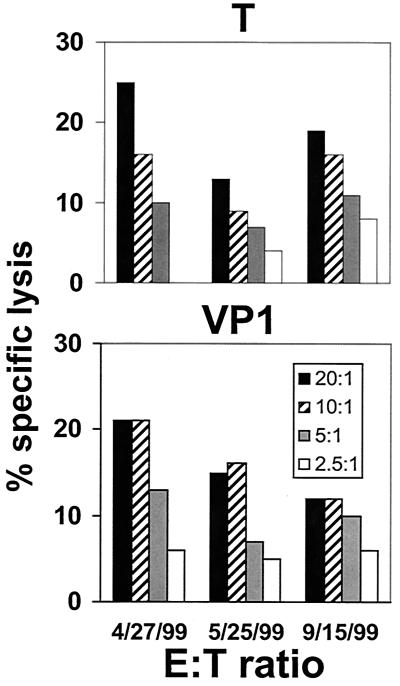
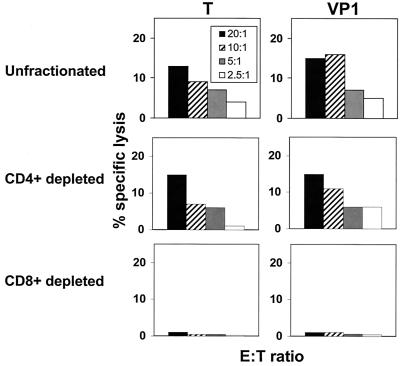
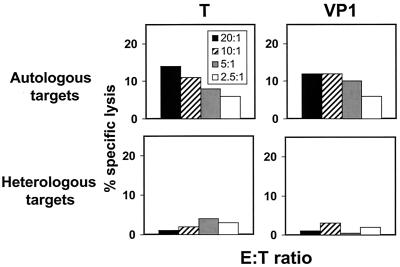
Progressive multifocal leukoencephalopathy (PML) is a demyelinating disease of the central nervous system caused by a reactivation of the polyomavirus JC (JCV) within a setting of immunosuppression. The nature of the immune response that contains replication of this virus is unknown. We have explored JCV-specific cellular immune responses in patients with PML and control subjects. JCV antigen-stimulated peripheral blood mononuclear cells (PBMC) of four human immunodeficiency virus (HIV)-infected patients who were survivors of PML and one HIV-uninfected patient recently diagnosed with PML lysed autologous B-lymphoblastoid cell lines expressing either the JCV T regulatory protein or the VP1 major capsid protein. This lysis was mediated by CD8(+) T lymphocytes and was major histocompatibility complex class I restricted. These cells were therefore cytotoxic T lymphocytes (CTL). JCV-specific CTL could not be detected in PBMC of three HIV-infected PML patients who had progressive neurologic disease and an eventual fatal outcome. These data suggest that the JCV-specific cellular immune response may play a crucial role in the containment of PML. This finding may also prove useful as a favorable prognostic marker in the clinical management of these patients.
Figures
References
-
- Achim C L, Wiley C A. Expression of major histocompatibility complex antigens in the brains of patients with progressive multifocal leukoencephalopathy. J Neuropathol Exp Neurol. 1992;51:257–263. - PubMed
-
- Ammassari A, Cingolani A, Pezzotti P, De Luca D A, Murri R, Giancola M L, Larocca L M, Antinori A. AIDS-related focal brain lesions in the era of highly active antiretroviral therapy. Neurology. 2000;55:1194–1200. - PubMed
-
- Berner B, Krieter D H, Rumpf K W, Grunewald R W, Beuche W, Weber T, Muller G A. Progressive multifocal leukoencephalopathy in a renal transplant patient diagnosed by JCV-specific DNA amplification and an intrathecal humoral immune response to recombinant virus protein 1. Nephrol Dial Transplant. 1999;14:462–465. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
