

Clinical results of the transjugular intrahepatic portosystemic shunt (TIPS) for the treatment of variceal bleeding
- PMID: 11242805
- PMCID: PMC4531767
- DOI: 10.3904/kjim.2000.15.3.179
Clinical results of the transjugular intrahepatic portosystemic shunt (TIPS) for the treatment of variceal bleeding
Abstract
Background: Transjugular intrahepatic portosystemic shunt (TIPS) has been popularized for the treatment of refractory variceal bleeding. The aim of this study was to assess the safety and long-term effect of TIPS in the treatment of variceal bleeding that is not controlled with pharmacological and endoscopic treatment.
Methods: Thirty-six patients who underwent transjugular intrahepatic portosystemic shunt (TIPS) due to refractory variceal bleeding were included in the study. The effectiveness of portal decompression and bleeding control was evaluated. Upper gastrointestinal endoscopy was performed to analyse the degree of varices and portal hypertensive gastropathy (PHG) before TIPS procedure and one to three weeks after TIPS. Angiography was performed in surviving patients, if bleeding recurred, or if ultrasonography or endoscopy suggested stent dysfunction.
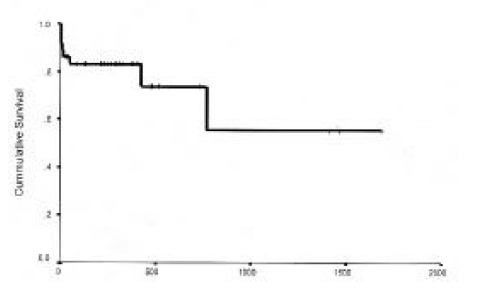
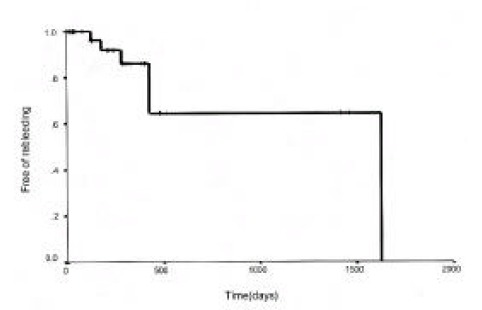
Results: TIPS were successfully placed in 36 of 38 patients (94.6%). TIPS achieved hemostasis of variceal bleeding in 34 patients (94.4%). Portal venous pressure decreased from an initial average of 28.7 +/- 7.9 to 23.2 +/- 9.4 mmHg after TIPS (p < 0.05). The portosystemic pressure gradient was significantly decreased from 15.5 +/- 6.3 to 7.8 +/- 4.1 mmHg (p < 0.01). The degree of esophagogastric varices and PHG was significantly improved after TIPS. The total length of follow-up was from one day to 54 months (mean: 355 days). The actuarial probability of survival was 83% at one year and 74% at two years. Overall, 16 episodes of stent dysfunction were diagnosed during follow-up. Stent revision by means of angioplasty was successfully performed in 14 of these episodes.
Conclusion: TIPS is an effective and reliable nonoperative means of lowering portal pressure. This procedure has proved useful in the management of acute variceal bleeding refractory to endoscopic treatment. Surveillance by ultrasonography, endoscopy, and angiographic intervention is useful for the maintenance of shunt patency.
Figures



References
-
- Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology. 1981;80:800–809. - PubMed
-
- D’Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension: a meta-analytic review. Hepatology. 1995;22:332–354. - PubMed
-
- de Dombal FT, Clarke JR, Clamp SE, Malizia G, Kotwal MR, Morgan AG. Prognostic factors in upper G.I. bleeding. Endoscopy. 1986;18(Suppl 2):6–10. - PubMed
-
- Cello JP, Grendell JH, Crass RA, Trunkey DD, Cobb EE, Heilbron DC. Endoscopic sclerotherapy versus portacaval shunt in patients with severe cirrhosis and variceal hemorrhage. N Engl J Med. 1984;311:1589–1594. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical