

Editorial
doi: 10.1136/heart.85.4.365.
Acute aortic syndrome
- PMID: 11250953
- PMCID: PMC1729697
- DOI: 10.1136/heart.85.4.365
Item in Clipboard
Editorial
Acute aortic syndrome
Heart.
2001 Apr.
No abstract available
Figures
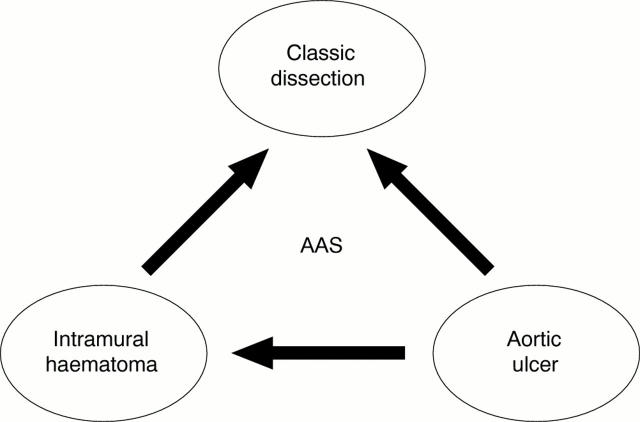
Acute aortic syndrome (AAS). Arrows indicate the possible progression of each of these aortic lesions.
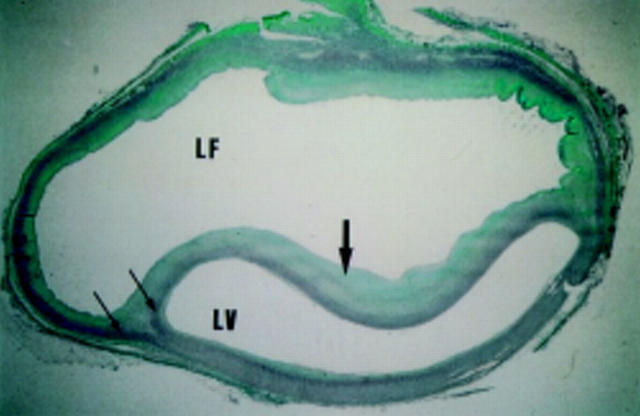
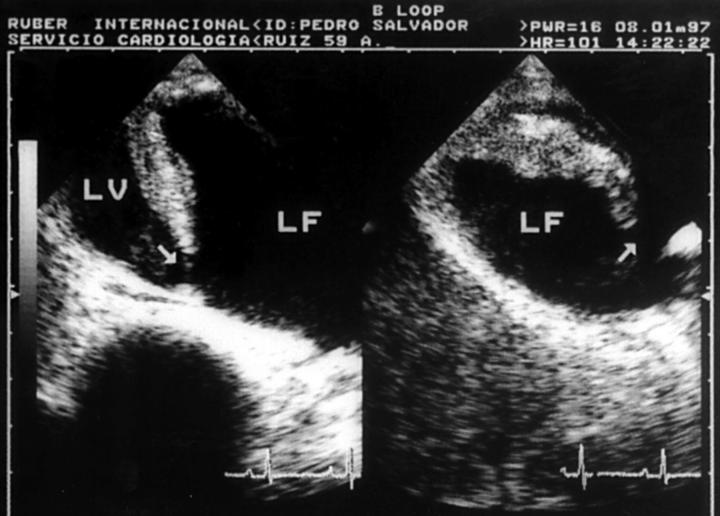
Histological section (Mason's technique) from a patient with aortic dissection. Muscle is stained in red and collagen in green. The aortic media (stained in red) is partitioned in two (arrows); one forms part of the dissection flap, the other forms the outer wall of the false channel. Large arrow indicates the dissection flap. LF, false lumen; LV, true lumen.

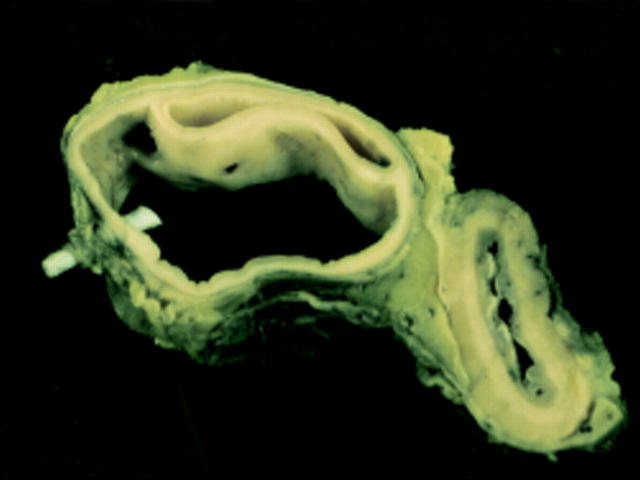
Anatomic specimen from a patient with type A aortic dissection. The entrance tear in the ascending aorta is clearly visible (arrow).
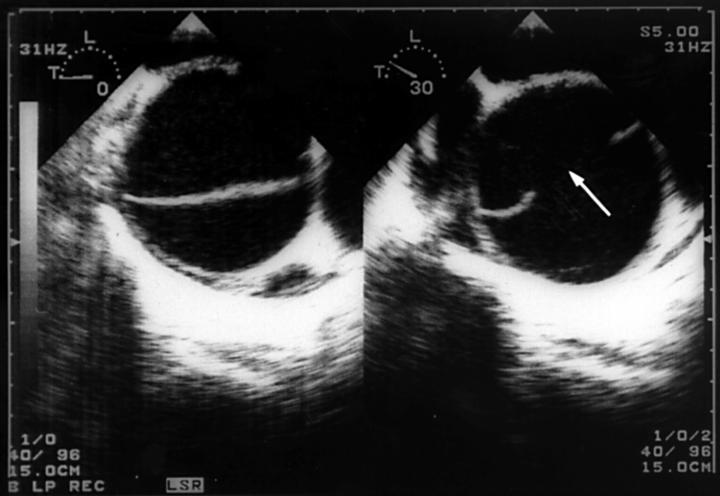
Transoesophageal echocardiographic study illustrating the double channel aorta and dissection flap (left panel), and the entrance tear (arrow) in the ascending aorta (right panel). Transversal planes.
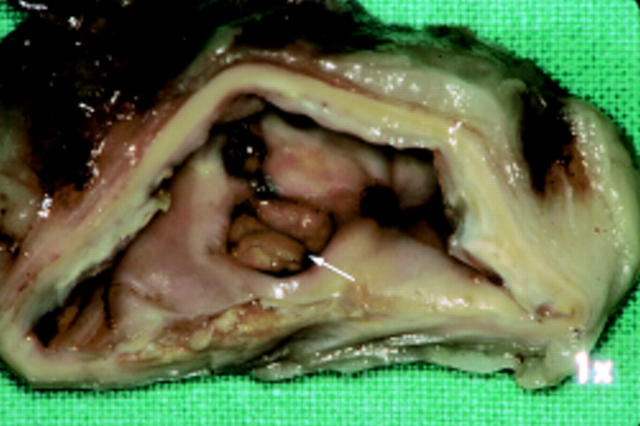
Anatomical cross section of the descending thoracic aorta. The ostium of an intercostal artery sectioned by the dissecting haematoma is clearly visible. A small hole in the dissection flap will permit blood flow between false and true aortic lumens.
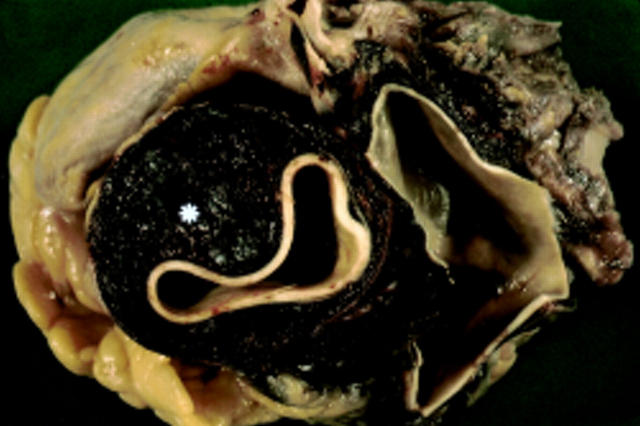
Anatomical cross section of the ascending aorta. An intramural aortic haematoma can be observed (asterisk).
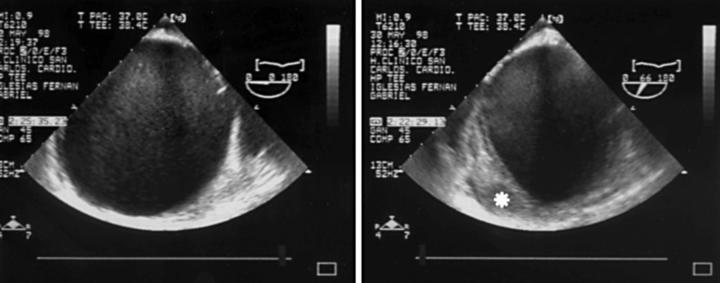
Transoesophageal echocardiographic study of a patient with a dilated aorta (left panel) and a crescent shaped thickening (asterisk) of the anterolateral wall of the aortic root that corresponds to an aortic intramural haematoma. Transverse planes.

Histological section (Mason's technique) of a patient with intramural haematoma. Splitting of the aortic media by a haematoma (asterisk) is well documented.
Anatomical cross section of the descending thoracic aorta. A penetrating atherosclerotic aortic ulcer is indicated by an arrow.

Transoesophageal echocardiographic study of a patient with an aortic ulcer (asterisk) in the descending thoracic aorta (AO). Longitudinal plane.
Transoesophageal echocardiographic scans in a patient with a limited acute aortic dissection secondary to aortic ulceration. A thick, calcified, irregular flap can be seen. Longitudinal planes. Arrow, entrance tear, LF, false lumen, LV, true lumen.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources