

The echocardiographic diagnosis of totally anomalous pulmonary venous connection in the fetus
- PMID: 11250972
- PMCID: PMC1729686
- DOI: 10.1136/heart.85.4.433
The echocardiographic diagnosis of totally anomalous pulmonary venous connection in the fetus
Abstract
Background: Infants with isolated totally anomalous pulmonary venous return often present severely decompensated, such that they are at high risk for surgical repair. On the other hand, if surgical repair can be safely accomplished, the outlook is usually good. Thus prenatal diagnosis would be expected to improve the prognosis for the affected child.
Objective: To describe the features of isolated totally anomalous pulmonary venous drainage in the fetus.
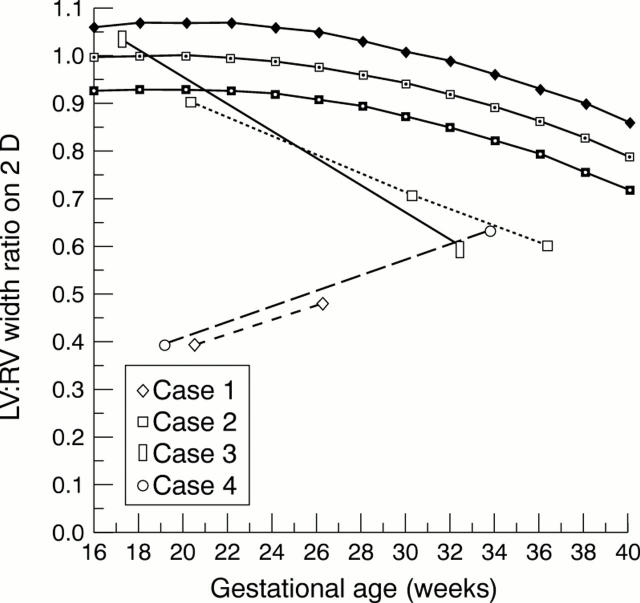
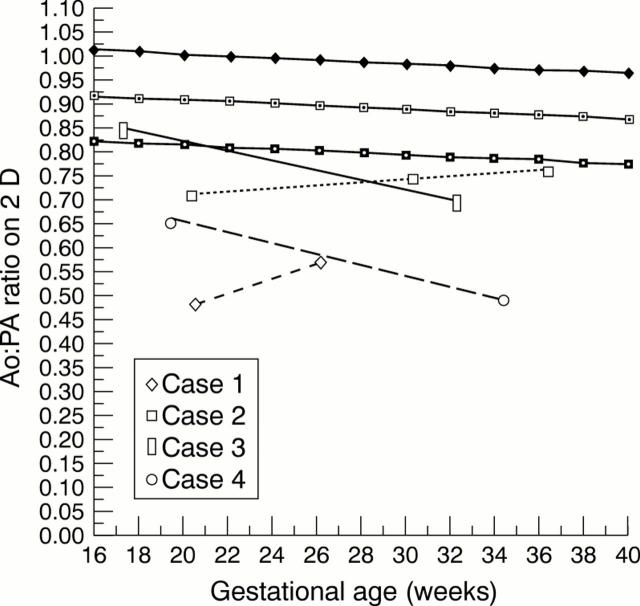
Design: Four fetuses with isolated totally anomalous pulmonary venous connection were identified and the echocardiographic images reviewed. Measurements of the atrial and ventricular chambers and both great arteries were made and compared with normal values.
Setting: Referral centre for fetal echocardiography.
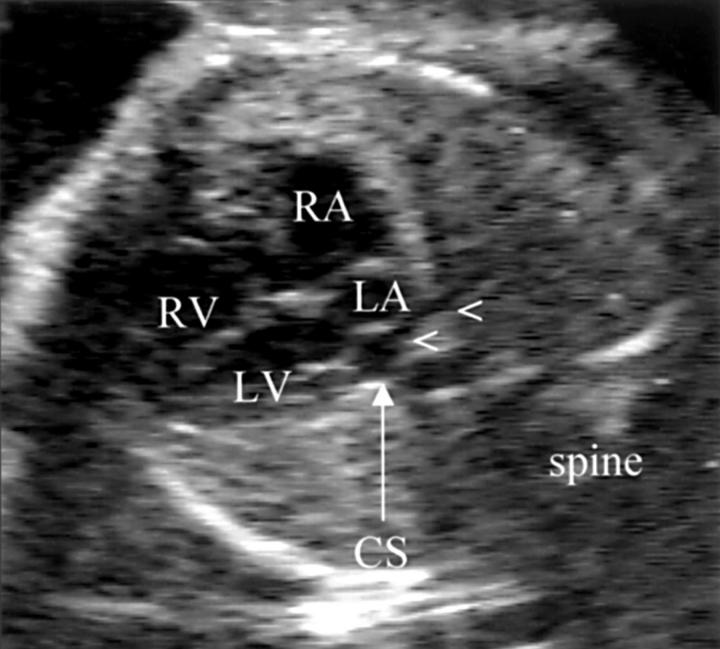
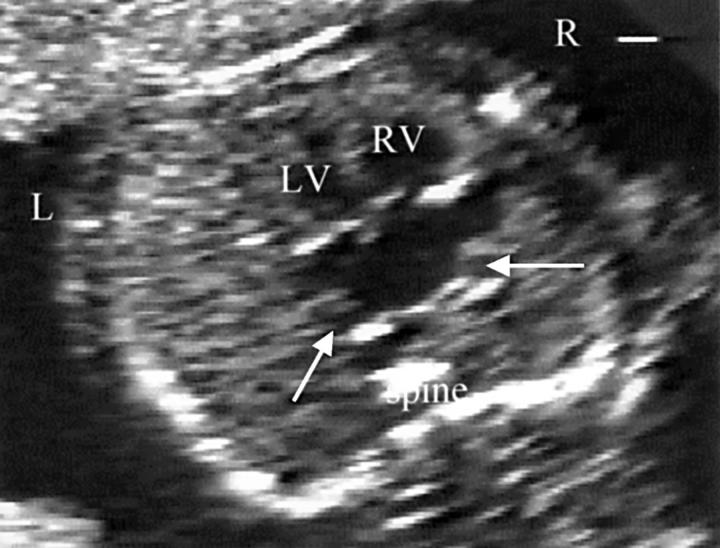
Results: There were two cases of drainage to the coronary sinus, one to the right superior vena cava, and one to the inferior vena cava. Right heart dilatation relative to left heart structures was a feature of two cases early on, and became evident in some ratios late in pregnancy in the remaining two.
Conclusions: Ventricular and great arterial disproportion in the fetus can indicate a diagnosis of totally anomalous pulmonary venous connection above the diaphragm. However, in the presence of an atrial septal defect or with infradiaphragmatic drainage, right heart dilatation may not occur until late in pregnancy. The diagnosis of totally anomalous pulmonary venous drainage in fetal life can only be reliably excluded by direct examination of pulmonary venous blood flow entering the left atrium on colour or pulsed flow mapping.
Figures


Similar articles
-
Fetal echocardiography in detecting anomalous pulmonary venous connection: four false positive cases.Br Heart J. 1995 Apr;73(4):355-8. doi: 10.1136/hrt.73.4.355. Br Heart J. 1995. PMID: 7756069 Free PMC article.
-
Prenatal diagnosis of a mixed type of total anomalous pulmonary venous return.Fetal Diagn Ther. 2010;27(2):118-20. doi: 10.1159/000279330. Epub 2010 Jan 27. Fetal Diagn Ther. 2010. PMID: 20110650
-
Prenatal diagnosis of isolated total anomalous pulmonary venous connection: a series of 10 cases.Ultrasound Obstet Gynecol. 2013 Mar;41(3):291-7. doi: 10.1002/uog.11186. Ultrasound Obstet Gynecol. 2013. PMID: 22605531
-
Prenatal diagnoses of an uncommon isolated obstructed supracardiac total anomalous pulmonary venous connection: Case report and review of the literature (CARE compliant).Medicine (Baltimore). 2017 Feb;96(5):e6061. doi: 10.1097/MD.0000000000006061. Medicine (Baltimore). 2017. PMID: 28151919 Free PMC article. Review.
-
The levoatriocardinal vein: morphology and echocardiographic identification of the pulmonary-systemic connection.J Am Coll Cardiol. 1995 Oct;26(4):995-1001. doi: 10.1016/0735-1097(95)00283-X. J Am Coll Cardiol. 1995. PMID: 7560630 Review.
Cited by
-
The impact of fetal echocardiography on the prevalence of liveborn congenital heart disease.Pediatr Cardiol. 2006 Jul-Aug;27(4):465-72. doi: 10.1007/s00246-006-1291-6. Epub 2006 Jul 6. Pediatr Cardiol. 2006. PMID: 16830077 Review.
-
Prenatal diagnosis and postnatal verification in fetuses with total anomalous pulmonary venous connection.Front Pediatr. 2023 Jun 7;11:1206032. doi: 10.3389/fped.2023.1206032. eCollection 2023. Front Pediatr. 2023. PMID: 37351315 Free PMC article.
-
Accuracy of prenatal screening for congenital heart disease in population: A retrospective study in Southern France.PLoS One. 2020 Oct 5;15(10):e0239476. doi: 10.1371/journal.pone.0239476. eCollection 2020. PLoS One. 2020. PMID: 33017437 Free PMC article.
-
Totally anomalous pulmonary venous drainage - supracardiac type: ultrasound assessment of anatomically determined stenosis of the vertical vein collecting pulmonary venous return and Ultrasound diagnosis of pulmonary sling with proximal stenosis of left pulmonary artery and patent arterial duct.J Ultrason. 2013 Jun;13(53):233-4. doi: 10.15557/JoU.2013.0024. Epub 2013 Jun 30. J Ultrason. 2013. PMID: 26672399 Free PMC article. No abstract available.
-
Fetal Pulmonary Venous Return: From Basic Research to the Clinical Value of Doppler Assessment.Pediatr Cardiol. 2023 Oct;44(7):1419-1437. doi: 10.1007/s00246-023-03244-4. Epub 2023 Jul 28. Pediatr Cardiol. 2023. PMID: 37505268 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical