

Pathophysiology of fluid imbalance
- PMID: 11255592
- PMCID: PMC3226173
- DOI: 10.1186/cc968
Pathophysiology of fluid imbalance
Abstract
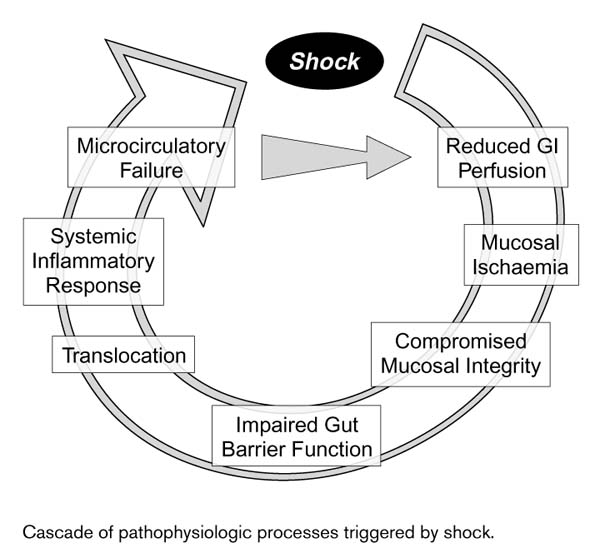
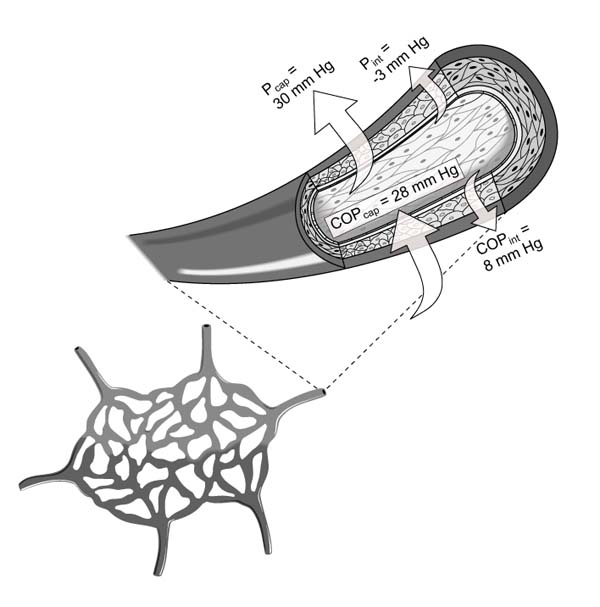
Fluid imbalance can arise due to hypovolemia, normovolemia with maldistribution of fluid, and hypervolemia. Trauma is among the most frequent causes of hypovolemia, with its often profuse attendant blood loss. Another common cause is dehydration, which primarily entails loss of plasma rather than whole blood. The consequences of hypovolemia include reduction in circulating blood volume, lower venous return and, in profound cases, arterial hypotension. Myocardial failure may result from increased myocardial oxygen demand in conjunction with reduced tissue perfusion. Finally, anaerobic metabolism due to reduced perfusion may produce acidosis and, together with myocardial dysfunction, precipitate multi-organ failure. The splanchnic organs are particularly susceptible to the deleterious effects of hypotension and hypovolemic shock, and these effects, depending upon their duration and severity, may be irreversible despite restoration of normovolemia by fluid administration. Patient monitoring in the intensive care unit typically relies upon central venous pressure devices, whereas the primary focus in the operating theater is blood volume deficit estimated from suction devices. However, estimates of intraoperative blood loss can be inaccurate, potentially leading to inappropriate fluid management. Normovolemia with maldistribution of fluid can be encountered in shock-specific microcirculatory disorders secondary to hypovolemia, as well as pain and stress. Consequent vasoconstriction and reduced tissue driving pressure, as well as leukocyte and platelet adhesion, and liberation of humoral and cellular mediators, may impair or abolish blood flow in certain areas. The localized perfusion deficit may contribute to multi-organ failure. Choice of resuscitation fluid may be important in this context, since some evidence suggests that at least certain colloids might be helpful in diminishing post-ischemic microvascular leukocyte adherence. Excessive volume administration may lead to fluid overload and associated impairment of pulmonary function. However, entry of fluid into the lungs may also be facilitated by increased vascular permeability in certain pathologic conditions, especially sepsis and endotoxemia, even in the absence of substantially rising hydrostatic pressure. Another condition associated with elevated vascular permeability is systemic capillary leak syndrome. The chief goal of fluid management, based upon current understanding of the pathophysiology of fluid imbalance, should be to ensure adequate oxygen delivery by optimizing blood oxygenation, perfusion pressure, and circulating volume.
Figures
References
-
- Burri C, Beck H, Ecke H, Unfallchirurgie, edn 3. Berlin: Springer Verlag, 1982.
-
- Meβmer K. Intestinal factors in shock: intestinal circulation. Langenbecks Arch Chir. 1967;319:890–909. - PubMed
-
- Oud L, Kruse JA. Progressive gastric intramucosal acidosis follows resuscitation from hemorrhagic shock. Shock. 1996;6:61–65. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
