

An impairment in sniffing contributes to the olfactory impairment in Parkinson's disease
- PMID: 11259673
- PMCID: PMC31195
- DOI: 10.1073/pnas.071061598
An impairment in sniffing contributes to the olfactory impairment in Parkinson's disease
Abstract
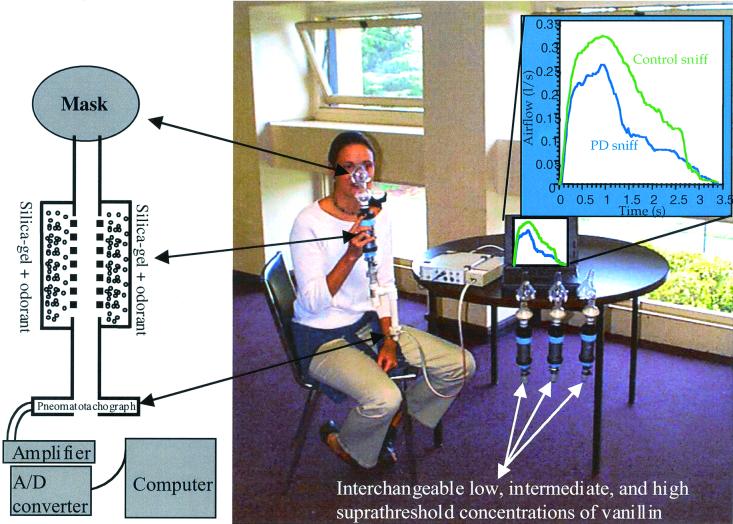
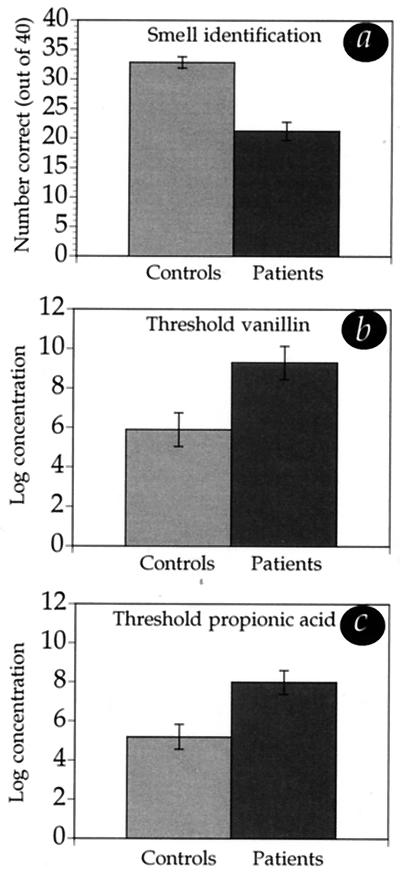
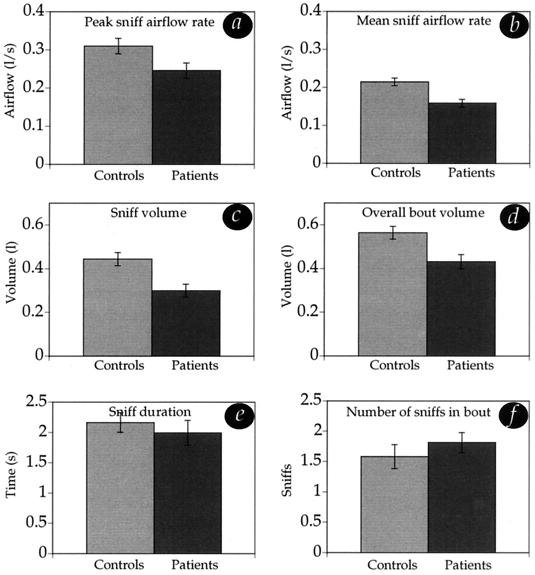
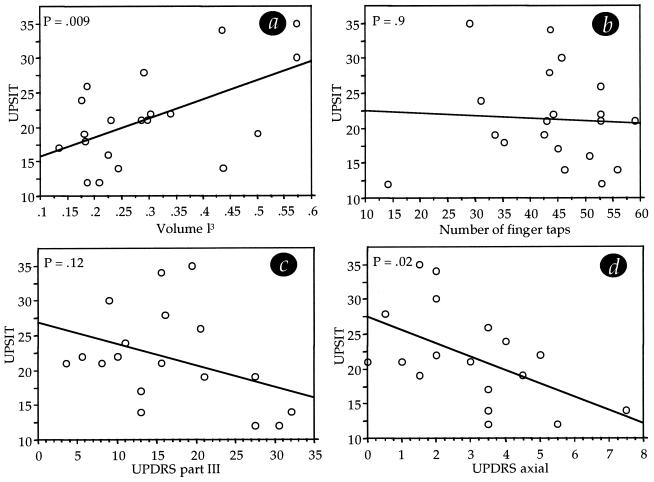
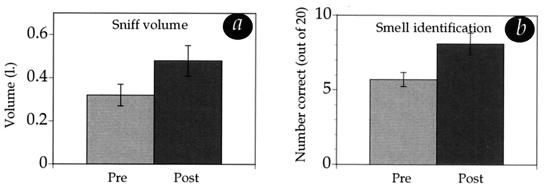
Although the presence of an olfactory impairment in Parkinson's disease (PD) has been recognized for 25 years, its cause remains unclear. Here we suggest a contributing factor to this impairment, namely, that PD impairs active sniffing of odorants. We tested 10 men and 10 women with clinically typical PD, and 20 age- and gender-matched healthy controls, in four olfactory tasks: (i) the University of Pennsylvania smell identification test; (ii and iii) detection threshold tests for the odorants vanillin and propionic acid; and (iv) a two-alternative forced-choice detection paradigm during which sniff parameters (airflow peak rate, mean rate, volume, and duration) were recorded with a pneomatotachograph-coupled spirometer. An additional experiment tested the effect of intentionally increasing sniff vigor on olfactory performance in 20 additional patients. PD patients were significantly impaired in olfactory identification (P < 0.0001) and detection (P < 0.007). As predicted, PD patients were also significantly impaired at sniffing, demonstrating significantly reduced sniff airflow rate (P < 0.01) and volume (P < 0.002). Furthermore, a patient's ability to sniff predicted his or her performance on olfactory tasks, i.e., the more poorly patients sniffed, the worse their performance on olfaction tests (P < 0.009). Finally, increasing sniff vigor improved olfactory performance in those patients whose baseline performance had been poorest (P < 0.05). These findings implicate a sniffing impairment as a component of the olfactory impairment in PD and further depict sniffing as an important component of human olfaction.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
