

Review
doi: 10.1136/bjo.85.4.483.
Treatment of subfoveal choroidal neovascularisation in age related macular degeneration: focus on clinical application of verteporfin photodynamic therapy
Affiliations
- PMID: 11264143
- PMCID: PMC1723921
- DOI: 10.1136/bjo.85.4.483
Item in Clipboard
Review
Treatment of subfoveal choroidal neovascularisation in age related macular degeneration: focus on clinical application of verteporfin photodynamic therapy
Br J Ophthalmol.
2001 Apr.
No abstract available
Figures
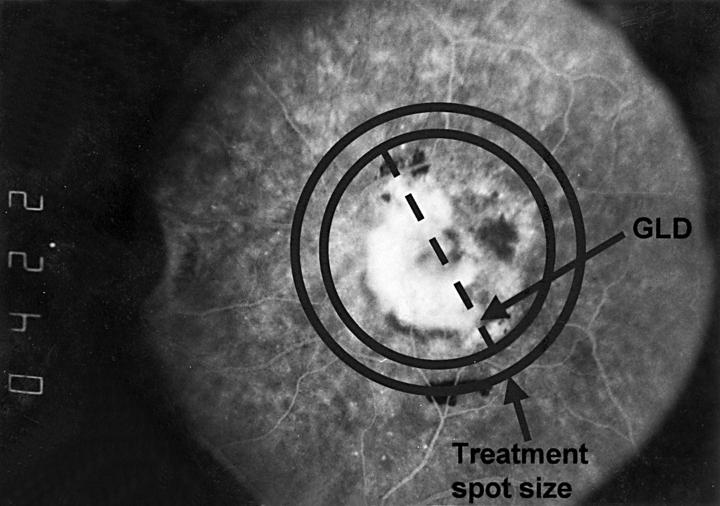
The spot size of the light used to activate verteporfin is calculated by measuring the greatest linear dimension (GLD) of the lesion on the retina from the fluorescein angiogram, adding 1000 µm to ensure a sufficient margin to cover the whole lesion. (Reproduced with permission from Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age related macular degeneration with verteporfin. Arch Ophthalmol 1999;117:1329-45.)
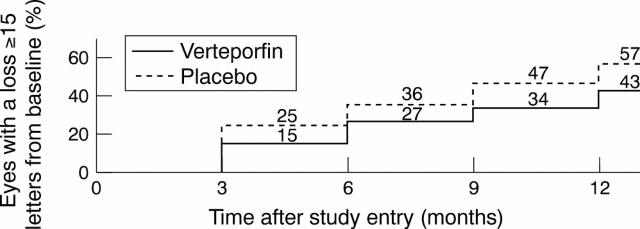
Kaplan-Meier estimates of the cumulative proportion of eyes treated with verteporfin or given placebo with moderate visual acuity loss (⩾15 letters or approximately ⩾3 lines) at each 3 month study visit over time during the first 12 months of the TAP investigation. (Reproduced with permission from Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age related macular degeneration with verteporfin. Arch Ophthalmol 1999;117:1329-45.)
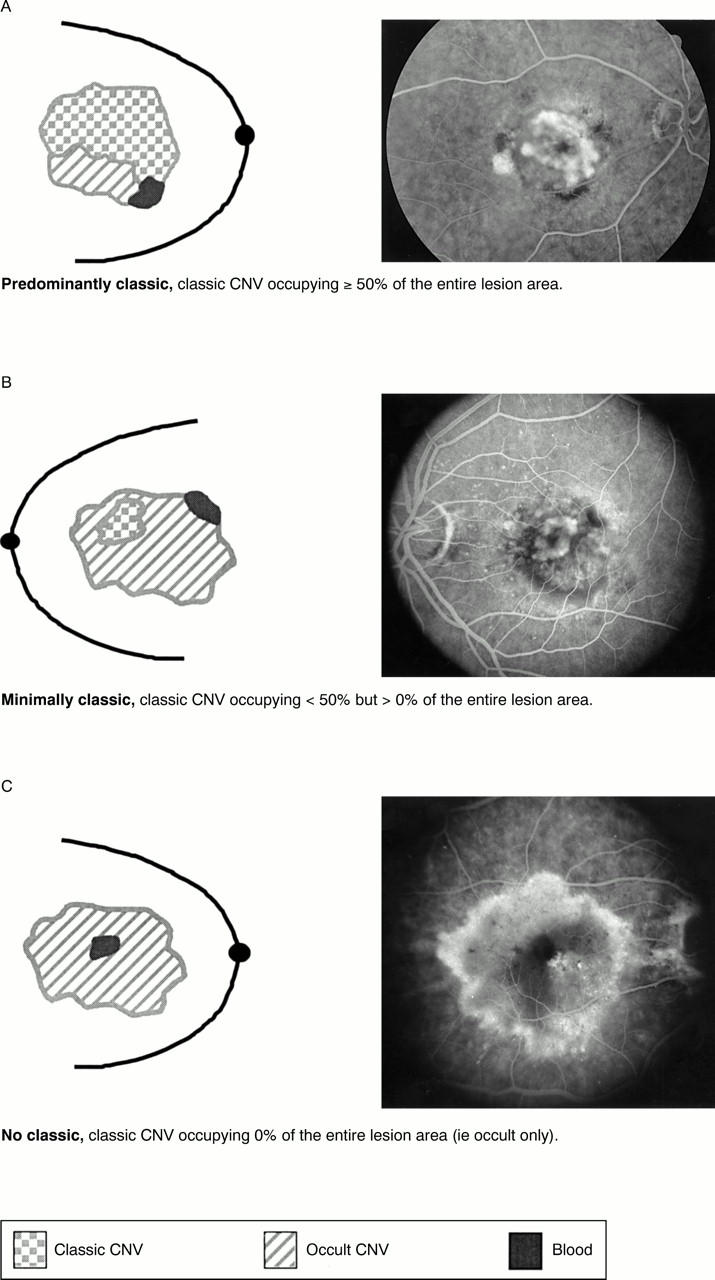
Schematic representations of mid phase angiographic examples of baseline lesion composition for a predominantly classic lesion (A), minimally classic lesion (B), and no classic, or occult only, lesion (C).
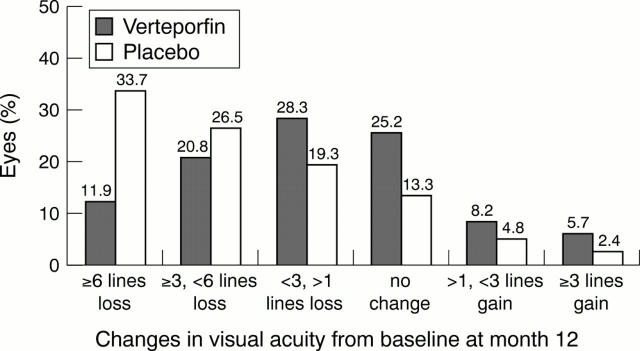
Distribution of changes in visual acuity from baseline at the month 12 examination of the TAP investigation for eyes with predominantly classic lesions.
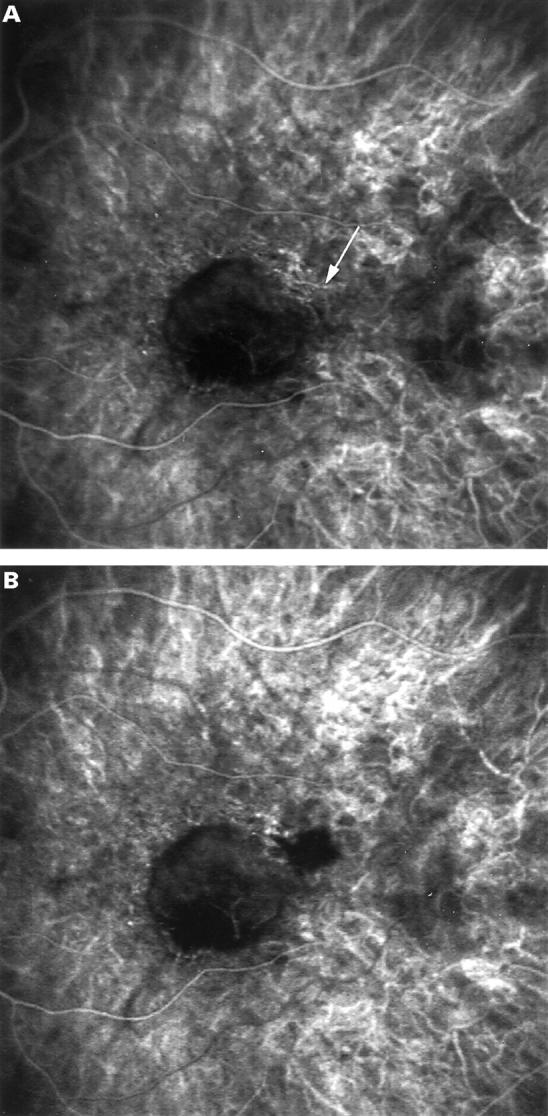
ICG guided feeder vessel photocoagulation. Very early phase ICG angiography at presentation (A) of patient with subfoveal occult CNV and visual acuity of 20/40. The early photographs show a horizontal choroidal vessel (arrow), intensely hyperfluorescent at the arterial choroidal phase, located in the superotemporal part of the posterior pole, outside of the foveal avascular zone. This vessel was considered to be the arterial feeder vessel of the CNV because it was only perfused for 3 seconds of the arterial phase, and was no longer visible thereafter. Furthermore, its perfusion was pulsatile, and its flow was in the opposite direction to that in the normal choroidal artery. The vessels below the feeding vessel were filling subsequently. Early phase of ICG angiography (B) immediately after focal laser photocoagulation of the feeder vessel shows hypofluorescence of the laser treated area superotemporal to the hypofluorescence of the neovascular lesion of the feeder vessel identified.
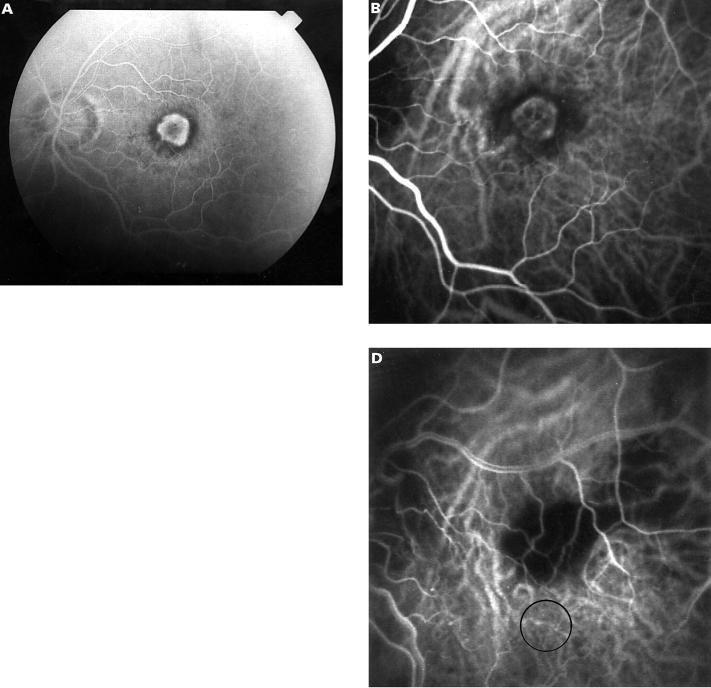
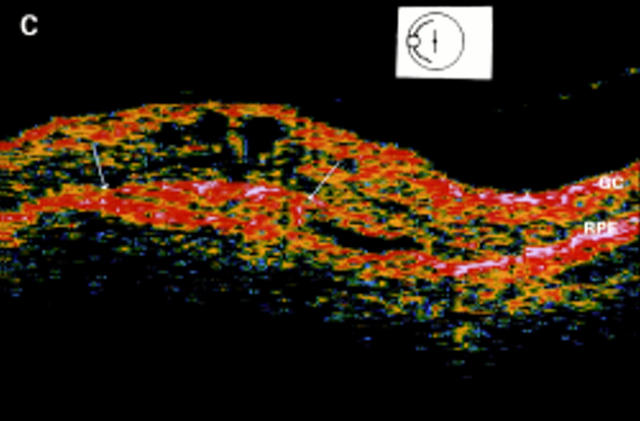
Limited foveal translocation. Fluorescein angiography at presentation (A) shows a small well defined foveal lesion involving the entire avascular zone. ICG angiography (B) discloses the subfoveal classic lesion in the same location as fluorescein angiography. OCT imaging (C) shows the normal hyperreflectivity of the ganglion cell layer in the inner retina (GC) and of the outer complex of retinal pigment epithelium, Bruch's membrane, and choriocapillaris (RPE). This later hyperreflectivity is a continuous layer, but a mushroom outgrowth is extending into the neurosensory retina (arrows). This aspect appears to correspond to the well defined choroidal lesion. ICG angiography (D) performed after surgically limited translocation and photocoagulation of the classic CNV shows that the laser treated area now lies next to the superotemporal retinal artery, outside of the fovea which is located away from the photocoagulated area (circle).
Limited foveal translocation. Fluorescein angiography at presentation (A) shows a small well defined foveal lesion involving the entire avascular zone. ICG angiography (B) discloses the subfoveal classic lesion in the same location as fluorescein angiography. OCT imaging (C) shows the normal hyperreflectivity of the ganglion cell layer in the inner retina (GC) and of the outer complex of retinal pigment epithelium, Bruch's membrane, and choriocapillaris (RPE). This later hyperreflectivity is a continuous layer, but a mushroom outgrowth is extending into the neurosensory retina (arrows). This aspect appears to correspond to the well defined choroidal lesion. ICG angiography (D) performed after surgically limited translocation and photocoagulation of the classic CNV shows that the laser treated area now lies next to the superotemporal retinal artery, outside of the fovea which is located away from the photocoagulated area (circle).
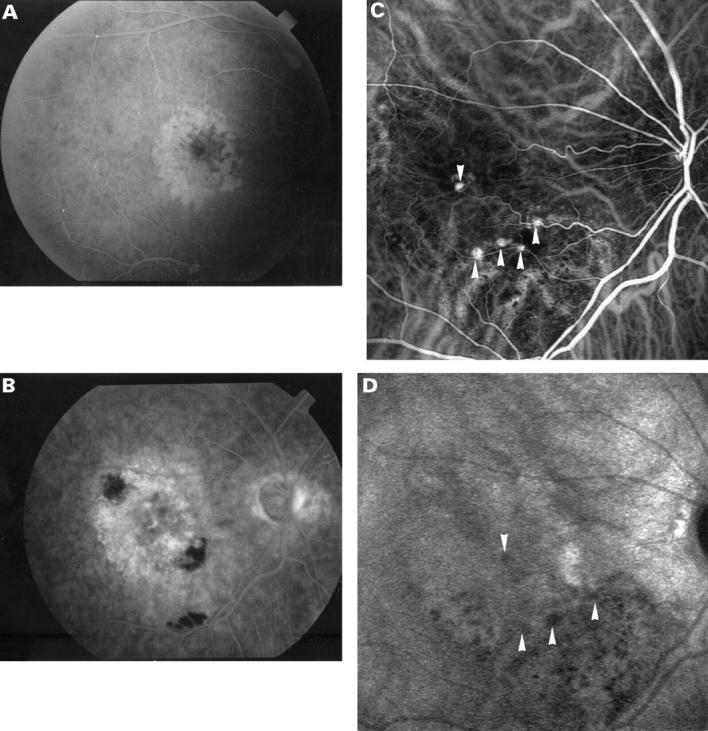
Radiation therapy for subfoveal occult CNV. Early phase fluorescein angiogram at presentation (A) shows small adjacent areas of hyperfluorescence and hypofluorescence involving the whole macula. Late phase fluorescein angiogram 1 month later (B) shows active occult new vessels with occurrence of retinal haemorrhage and subfoveal fluorescein leakage 2.5 MPS disc areas in size. No laser photocoagulation treatment could be considered and thus the patient was submitted to radiation therapy. Early phase ICG angiogram (C) performed 14 months after treatment demonstrates five areas of round, hyperfluorescent choroidal dilatation disseminated on the border of the remaining lesion (arrowheads). Later phase ICG angiogram (D) discloses the washout of some of the hyperfluorescent bulges (arrowheads)
Similar articles
-
Verteporfin : a review of its use in the management of subfoveal choroidal neovascularisation.Drugs. 2003;63(22):2521-54. doi: 10.2165/00003495-200363220-00016. Drugs. 2003. PMID: 14609361 Review.
-
Verteporfin therapy of subfoveal choroidal neovascularization in age-related macular degeneration: two-year results of a randomized clinical trial including lesions with occult with no classic choroidal neovascularization-verteporfin in photodynamic therapy report 2.Am J Ophthalmol. 2002 Jan;133(1):168-9. doi: 10.1016/s0002-9394(01)01237-5. Am J Ophthalmol. 2002. PMID: 11755871 Clinical Trial. No abstract available.
-
Retinal translocation and photodynamic therapy for age-related macular degeneration with classic choroidal neovascularization: a clinicopathologic case report.Retina. 2002 Dec;22(6):818-24. doi: 10.1097/00006982-200212000-00027. Retina. 2002. PMID: 12476118 No abstract available.
-
Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group.Arch Ophthalmol. 1999 Oct;117(10):1329-45. Arch Ophthalmol. 1999. PMID: 10532441 Clinical Trial.
-
Verteporfin ocular photodynamic therapy.Expert Opin Pharmacother. 2004 Jan;5(1):195-203. doi: 10.1517/14656566.5.1.195. Expert Opin Pharmacother. 2004. PMID: 14680447 Review.
Cited by
-
Verteporfin Photodynamic Therapy for the Treatment of Chorioretinal Conditions: A Narrative Review.Clin Ophthalmol. 2024 Jun 10;18:1701-1716. doi: 10.2147/OPTH.S464371. eCollection 2024. Clin Ophthalmol. 2024. PMID: 38881707 Free PMC article. Review.
-
Application and investigation of thrombopoiesis-stimulating agents in the treatment of thrombocytopenia.Ther Adv Hematol. 2023 Feb 27;14:20406207231152746. doi: 10.1177/20406207231152746. eCollection 2023. Ther Adv Hematol. 2023. PMID: 36865986 Free PMC article. Review.
-
Age-related macular degeneration.Ulster Med J. 2005 Sep;74(2):82-92. Ulster Med J. 2005. PMID: 16235759 Free PMC article. Review. No abstract available.
-
Verteporfin : a review of its use in the management of subfoveal choroidal neovascularisation.Drugs. 2003;63(22):2521-54. doi: 10.2165/00003495-200363220-00016. Drugs. 2003. PMID: 14609361 Review.
-
Giant neurosensory detachments associated with disciform lesions in neovascular age related macular degeneration.Br J Ophthalmol. 2003 Jun;87(6):795-6. doi: 10.1136/bjo.87.6.795-a. Br J Ophthalmol. 2003. PMID: 12770991 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical