

Cabergoline for levodopa-induced complications in Parkinson's disease
- PMID: 11279720
- PMCID: PMC8406784
- DOI: 10.1002/14651858.CD001518
Cabergoline for levodopa-induced complications in Parkinson's disease
Abstract
Background: Long term levodopa therapy in Parkinson's disease is associated with the development of motor complications including abnormal involuntary movements and a shortening response to each dose (wearing off phenomenon). It is thought that dopamine agonists can reduce the duration of immobile off periods and the need for levodopa therapy whilst maintaining or improving motor impairments and only minimally increasing dopaminergic adverse events.
Objectives: To compare the efficacy and safety of adjuvant cabergoline therapy versus placebo in patients with Parkinson's disease, already established on levodopa and suffering from motor complications.
Search strategy: Electronic searches of MEDLINE, EMBASE and the Cochrane Controlled Trials Register. Handsearching of the neurology literature as part of the Cochrane Movement Disorders Group's strategy. Examination of the reference lists of identified studies and other reviews. Contact with Pharmacia Upjohn Limited.
Selection criteria: Randomised controlled trials of cabergoline versus placebo in patients with a clinical diagnosis of idiopathic Parkinson's disease and long-term complications of levodopa therapy.
Data collection and analysis: Data was abstracted independently by the authors and differences settled by discussion. The outcome measures used included Parkinson's disease rating scales, levodopa dosage, off time measurements and the frequency of withdrawals and adverse events.
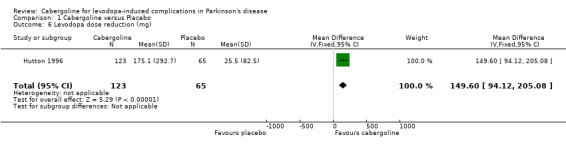
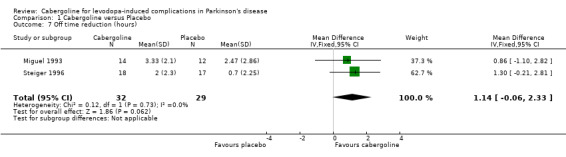
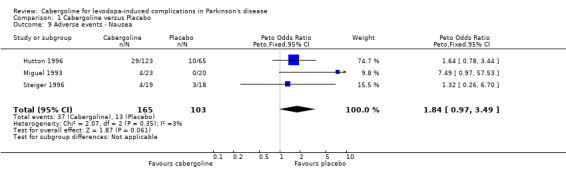
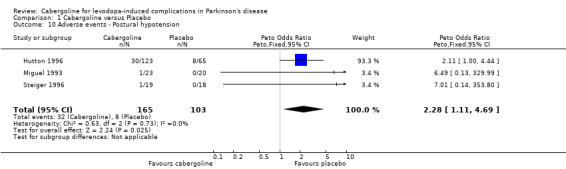
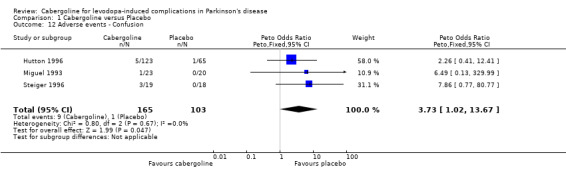
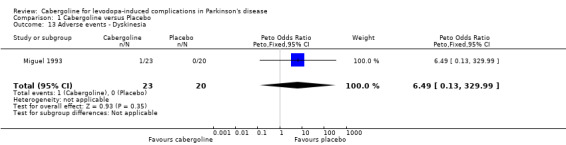
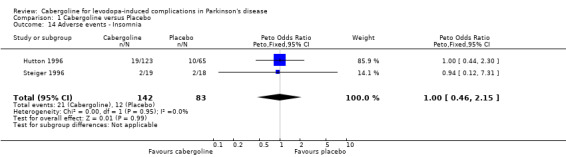
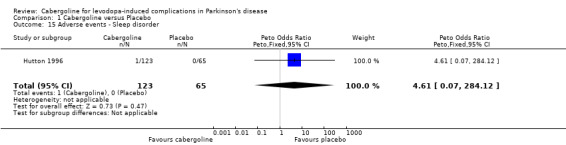
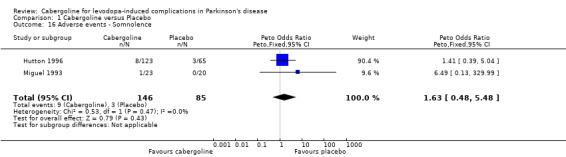
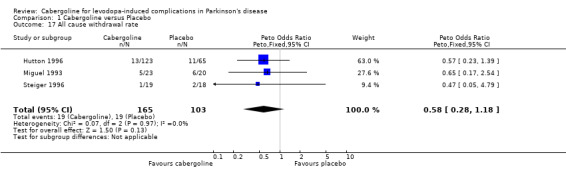
Main results: Cabergoline has been compared with placebo in two phase II (6 - 12 weeks) and one phase III randomised controlled trials (24 weeks). These were double-blind, parallel group, multicentre studies including 268 patients with Parkinson's disease and motor complications. The reduction of 1.14 hours (WMD; 95% CI -0.06, 2.33; p = 0.06) in off time in favour of cabergoline was not statistically significant. Inadequate data on dyskinesia was collected either on rating scales or as adverse event reporting to allow a conclusion to be drawn. A small but statistically significant advantage of cabergoline over placebo was seen in one study for UPDRS ADL (part II) score and UPDRS motor score. No such advantage was seen in one other study due to small numbers of patients and the comparatively low doses of cabergoline used. No significant differences in Schwab and England scale were seen in two studies. Levodopa dose reduction was significantly greater with cabergoline (WMD 149.6 mg/d; 95% CI 94.1, 205.1; p < 0.00001). There was a trend towards more dopaminergic adverse events with cabergoline but this did not reach statistical significance at the p < 0.01 level. However, there was a trend towards fewer withdrawals from cabergoline.
Reviewer's conclusions: In the management of the motor complications seen in Parkinson's disease, cabergoline can be used to reduce levodopa dose and modestly improve motor impairment and disability with an acceptable adverse event profile. These conclusions are based on, at best, medium term evidence.
Conflict of interest statement
CEC has received payment from Pharmacia Upjohn for lectures and attending meetings.
Figures

References
References to studies included in this review
Hutton 1996 {published and unpublished data}
-
- Ahlskog JE, Wright KF, Muenter MD, Adler CH. Adjunctive cabergoline therapy of Parkinson's disease: comparison with placebo and assessment of dose responses and duration of effect. Clinical Neuropharmacology 1996;19:202‐212. - PubMed
-
- Hutton JT, Koller WC, Ahlskog JE, et al. Multicentre, placebo‐controlled trial of cabergoline taken once daily in the treatment of Parkinson's disease. Neurology 1996;46:1062‐1065. - PubMed
Miguel 1993 {unpublished data only}
-
- Miguel F, Obeso JA, Olive Plana JM, Tolosa E, Villaueva Eusa JA, Dubini A, et al. Double‐blind parallel group study of the efficacy and tolerability of the cabergoline vs placebo in Parkinsonian patients with motor fluctuations. FCE Report: 21336/722i, Clinical Reference 29 1993.
Steiger 1996 {published data only}
-
- Steiger MJ, El‐Debas T, Anderson T, Findley LJ, Marsden CD. Double‐blind study of the activity and tolerability of cabergoline versus placebo in parkinsonains with motor fluctuations. Journal of Neurology 1996;243:68‐72. - PubMed
References to studies excluded from this review
Ahlskog 1994 {published data only}
-
- Ahlskog JE, Muenter MD, Maraganore DM, et al. Fluctuating Parkinson's disease. Treatment with the long‐acting dopamine agonist cabergoline. Archives of Neurology 1994;51:1236‐1241. - PubMed
Ahlskog 1996 {published data only}
-
- Ahlskog EJ, Wright KF, Muenter MD, Adler CH. Adjunctive cabergoline therapy of Parkinson's disease: comparison with placebo and assessment of dose responses and duration of effect. Clinical Neuropharmacology 1996;19:202‐212. - PubMed
Additional references
CONSORT 1996
-
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, Pitkin R, Rennie D, Schulz KF, Simel D, Stroup DF. Improving the quality of reporting of randomized controlled trials: the CONSORT statement.. Journal of the American Medical Association 1996;276(8):637‐639. - PubMed
Quinn 1986
-
- Quinn N, Critchley P, Parkes D, Marsden CD. When should levodopa be started?. Lancet 1986;ii:985‐986. - PubMed
Rajput 1984
-
- Rajput AH, Stern W, Laverty WH. Chronic low‐dose levodopa therapy in Parkinson's disease. Neurology 1984;34:991‐996. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources