

Is 'shared decision-making' feasible in consultations for upper respiratory tract infections? Assessing the influence of antibiotic expectations using discourse analysis
- PMID: 11281884
- PMCID: PMC5061443
- DOI: 10.1046/j.1369-6513.1999.00045.x
Is 'shared decision-making' feasible in consultations for upper respiratory tract infections? Assessing the influence of antibiotic expectations using discourse analysis
Abstract
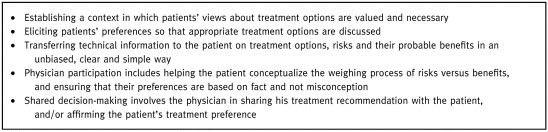
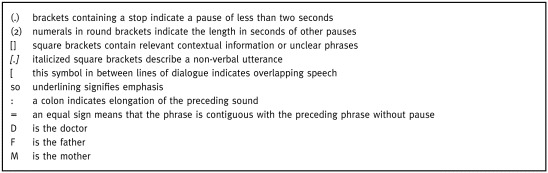
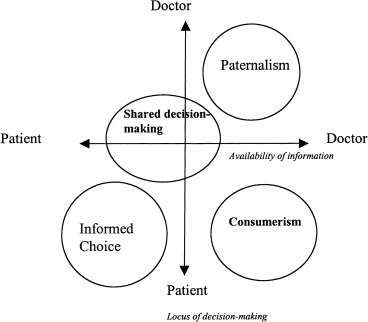
OBJECTIVES: To examine the discourse of consultations in which conflict occurs between parents and clinicians about the necessity of antibiotics to treat an upper respiratory tract infection. To appraise the feasibility of shared decision-making in such consultations. DESIGN: A qualitative study using discourse analysis techniques. SETTING: A general practice with 12 500 patients in an urban area of Cardiff, Wales. PARTICIPANTS: Two consultations were purposively selected from a number of audiotaped sessions. The consultations took place during normal clinics in which appointments are booked at 7-minute intervals. The practitioner is known to be interested in involving patients in treatment decisions. METHOD: Discourse analysis was employed to examine the consultation transcripts. This analysis was then compared with the theoretical competencies proposed for 'shared decision-making'. RESULTS: The consultations exhibit less rational strategies than those suggested by the shared decision-making model. Strong parental views are expressed (overtly and covertly) which seem derived from prior experiences of similar illnesses and prescribing behaviours. The clinician responds by emphasizing the 'normality' of upper respiratory tract infections and their recurrence, accompanied by expressions that antibiotic treatment is ineffective in 'viral' illness - the suggested diagnosis. The competencies of 'shared decision-making' are not exhibited. CONCLUSIONS: The current understanding of shared decision-making needs to be developed for those situations where there are dis-agreements due to the strongly held views of the participants. Clinicians have limited strategies in situations where patient treatment preferences are opposed to professional views. Dispelling 'misconceptions' by sharing information and negotiating agreed management plans are recommended. But it seems that communication skills, information content and consultation length have to receive attention if such strategies are to be employed successfully.
Figures

References
-
- Coulter A. Partnerships with patients: the pros and cons of shared clinical decision‐making. Journal of Health Services Research and Policy, 1997; 2 : 112 121. - PubMed
-
- Guadagnoli E & Ward P. Patient participation in decision‐making . Social Science and Medicine, 1998; 47 (3): 329 339. - PubMed
-
- Stewart M, Brown JB, Weston WW, McWinney IR, McWilliam CL, Freeman T. Patient Centred Medicine. Transforming the Clinical Method Thousand Oaks, CA: Sage Publications, 1995.
-
- Stewart M. Studies of health outcomes and patient‐centered communication . In: Stewart M, Brown JB, Weston WW, Mcwhinney IR, Mcwillima CL, Freeman TR, (eds) Patient‐centered Medicine. Thousand Oaks, CA: Sage Publications, 1995.
-
- Charles C, Gafni A, Whelan T. Shared decision‐making in the medical encounter: what does it mean? (Or it takes at least two to tango). Social Science and Medicine, 1997; 44 : 681 692. - PubMed
LinkOut - more resources
Full Text Sources
