

Replicative senescence of biliary epithelial cells precedes bile duct loss in chronic liver allograft rejection: increased expression of p21(WAF1/Cip1) as a disease marker and the influence of immunosuppressive drugs
- PMID: 11290556
- PMCID: PMC1891905
- DOI: 10.1016/S0002-9440(10)64089-8
Replicative senescence of biliary epithelial cells precedes bile duct loss in chronic liver allograft rejection: increased expression of p21(WAF1/Cip1) as a disease marker and the influence of immunosuppressive drugs
Abstract
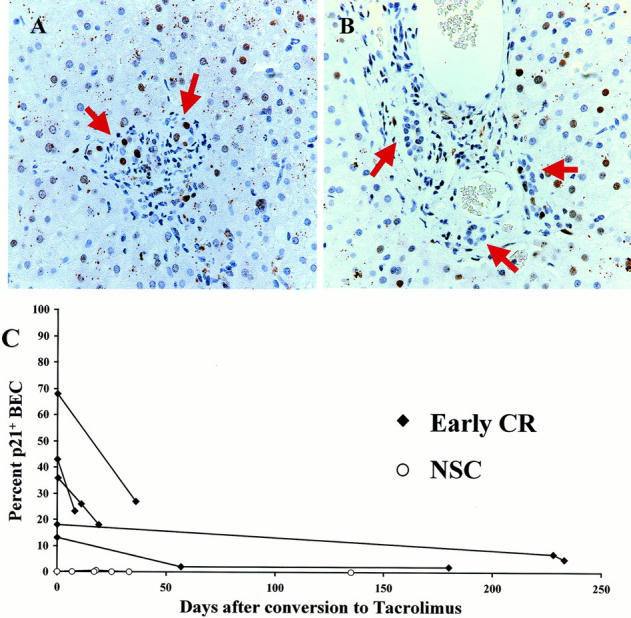
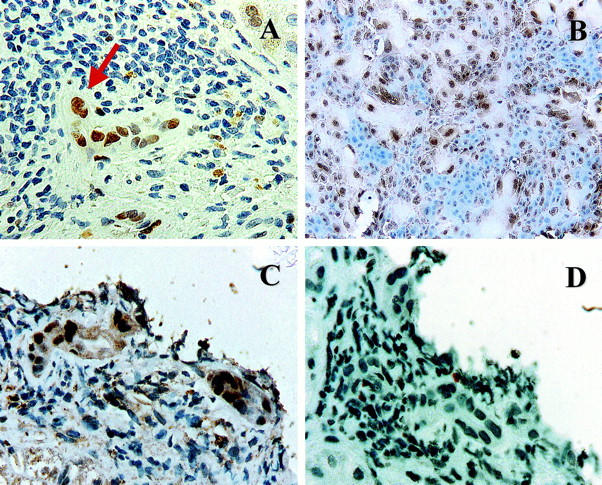
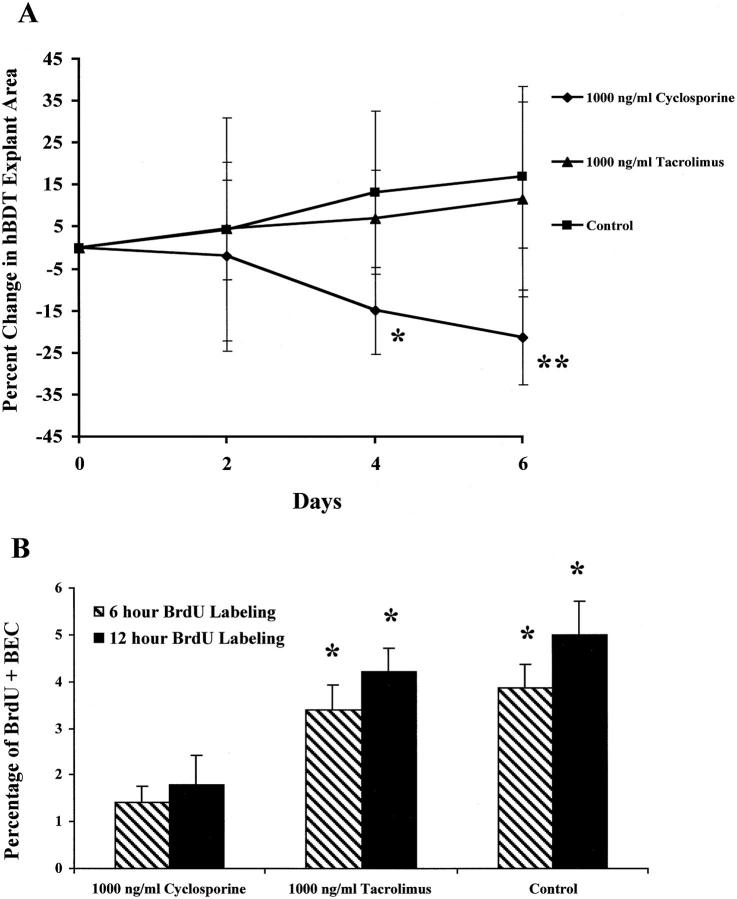
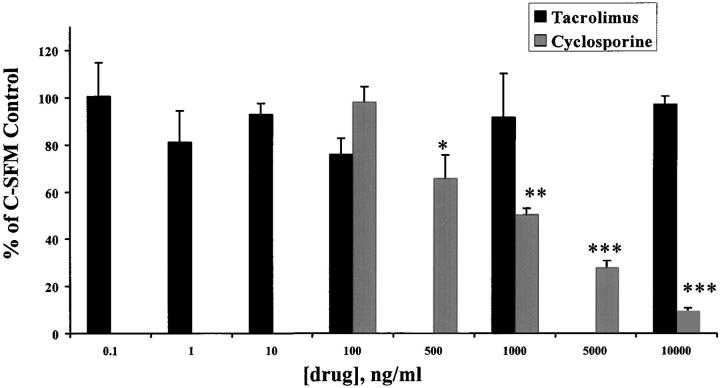
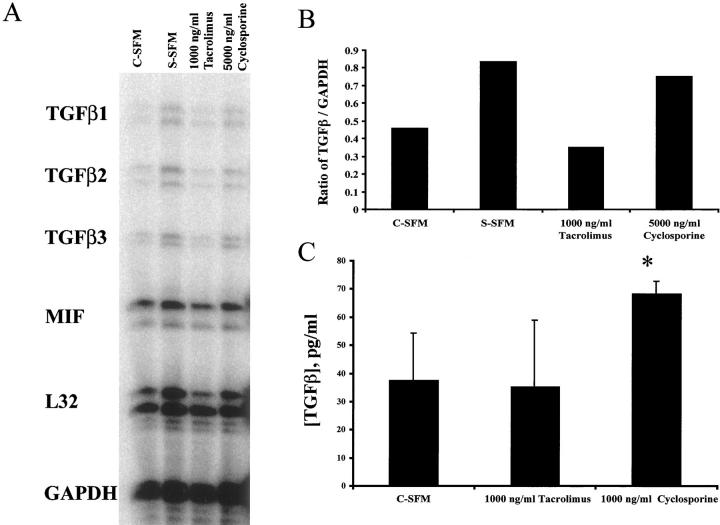
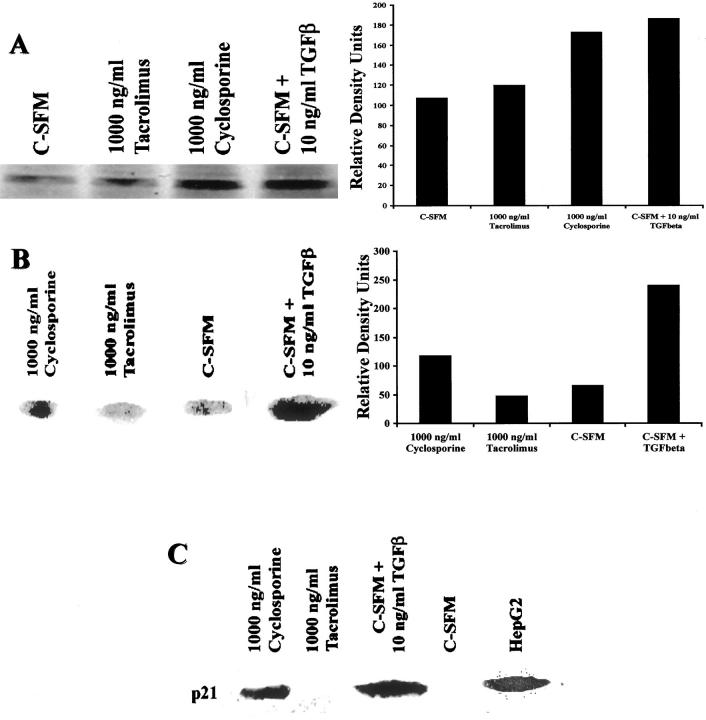
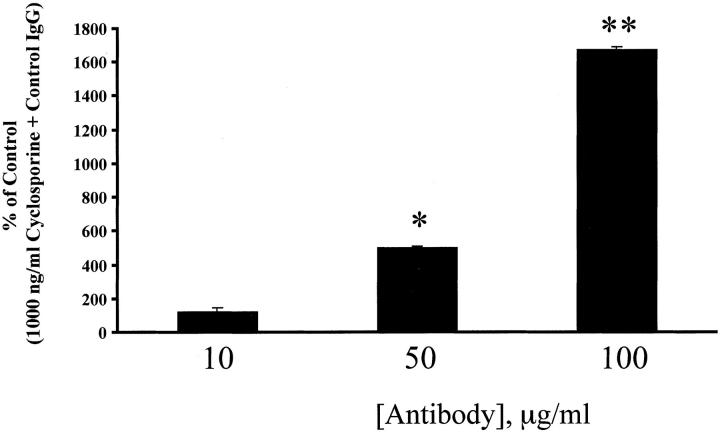
Early chronic liver allograft rejection (CR) is characterized by distinctive cytological changes in biliary epithelial cells (BECs) that resemble cellular senescence, in vitro, and precede bile duct loss. If patients suffering from early CR are treated aggressively, the clinical and histopathological manifestations of CR can be completely reversed and bile duct loss can be prevented. We first tested whether the senescence-related p21(WAF1/Cip1) protein is increased in BECs during early CR, and whether treatment reversed the expression. The percentage of p21+ BECs and the number of p21+ BECs per portal tract is significantly increased in early CR (26 +/- 17% and 3.6 +/- 3.1) compared to BECs in normal liver allograft biopsies or those with nonspecific changes (1 +/- 1% and 0.1 +/- 0.3; P: < 0.0001 and P: < 0.02), chronic hepatitis C (2 +/- 3% and 0.7 +/- 1; P: < 0.0001 and P: < 0.04) or obstructive cholangiopathy (7 +/- 7% and 0.7 +/- 0.6; P: < 0.006 and P: = 0.04). Successful treatment of early CR is associated with a decrease in the percentage of p21+ BECs and the number of p21+ BECs per portal tract. In vitro, nuclear p21(WAF1/Cip1) expression is increased in large and multinucleated BECs, and is induced by transforming growth factor (TGF)-beta. TGF-beta1 also increases expression of TGF-beta receptor II, causes phosphorylation of SMAD-2 and nuclear translocation of p21(WAF1/Cip1), which inhibits BEC growth. Because conversion from cyclosporine to tacrolimus is an effective treatment for early CR, we next tested whether these two immunosuppressive drugs directly influenced BEC growth in vitro. The results show that cyclosporine, but not tacrolimus, stimulates BEC TGF-beta1 production, which in turn, causes BEC mito-inhibition and up-regulation of nuclear p21(WAF1/Cip1). In conclusion, expression of the senescence-related p21(WAF1/Cip1) protein is increased in BECs during early CR and decreases with successful recovery. Replicative senescence accounts for the characteristic BEC cytological alterations used for the diagnosis of early CR and lack of a proliferative response to injury. The ability of cyclosporine to inhibit the growth of damaged BECs likely accounts for the relative duct sparing properties of tacrolimus.
Figures
References
-
- Freese DK, Snover DC, Sharp HL, Gross CR, Savick SK, Payne WD: Chronic rejection after liver transplantation: a study of clinical, histopathological and immunological features. Hepatology 1991, 13:882-891 - PubMed
-
- Hubscher SG, Buckels JA, Elias E, McMaster P, Neuberger J: Vanishing bile-duct syndrome following liver transplantation—is it reversible? Transplantation 1991, 51:1004-1010 - PubMed
-
- Lautenschlager I, Hockerstedt K, Jalanko H, Loginov R, Salmela K, Taskinen E, Ahonen J: Persistent cytomegalovirus in liver allografts with chronic rejection. Hepatology 1997, 25:190-194 - PubMed
-
- Blakolmer K, Seaberg EC, Batts K, Ferrell L, Markin R, Wiesner R, Detre K, Demetris A: Analysis of the reversibility of chronic liver allograft rejection implications for a staging schema. Am J Surg Pathol 1999, 23:1328-1339 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
