

Preventing recurrent depression using cognitive therapy with and without a continuation phase: a randomized clinical trial
- PMID: 11296099
- PMCID: PMC1307495
- DOI: 10.1001/archpsyc.58.4.381
Preventing recurrent depression using cognitive therapy with and without a continuation phase: a randomized clinical trial
Abstract
Background: Cognitive therapy (CT) may reduce depressive relapse and recurrence when patients learn and use the associated skills. Reported relapse and recurrence rates after CT discontinuation vary widely. The factors that determine when CT is preventive remain unidentified. We developed continuation-phase CT (C-CT) to teach responders skills to prevent relapse. This is the first randomized trial comparing CT with and without a continuation phase in responders to CT who were vulnerable, given their history of recurrent unipolar depression.
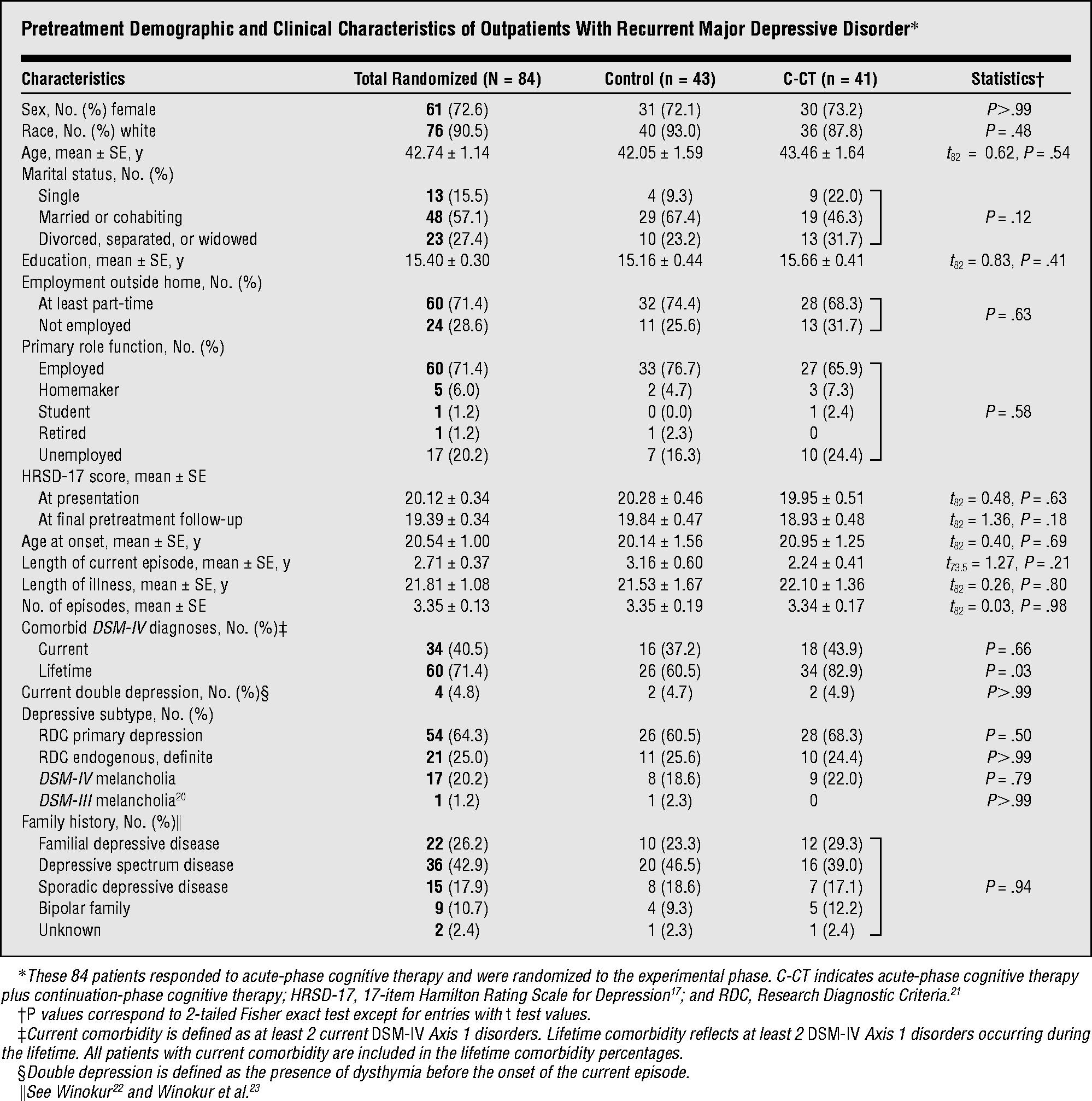
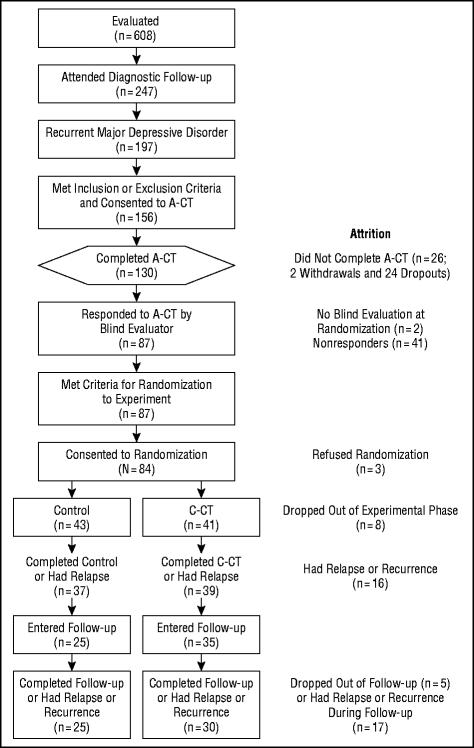
Methods: Patients aged 18 to 65 years (n = 156) with recurrent DSM-IV major depressive disorder (MDD) entered 20 sessions of acute-phase CT (A-CT). Unmedicated responders (ie, no MDD and 17-item Hamilton Rating Scale for Depression score < or =9; n = 84) were randomized to either 8 months (10 sessions) of C-CT or control (evaluation without CT). Follow-up lasted an additional 16 months. A clinician blind to assignment evaluated relapse and recurrence (ie, DSM-IV MDD).
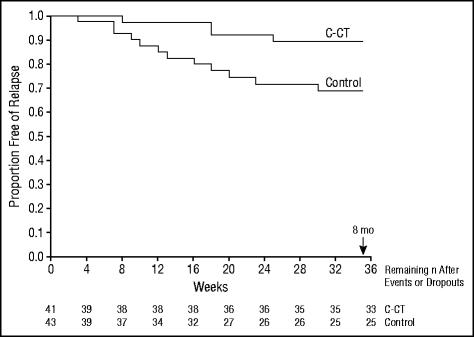
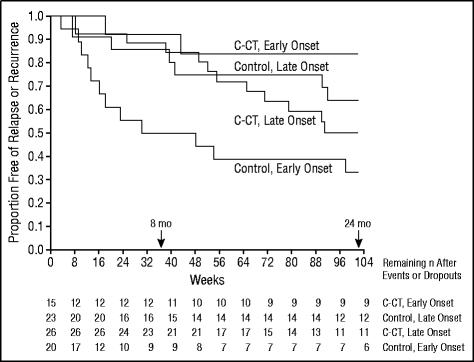
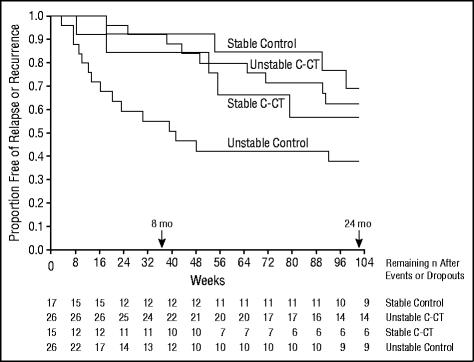
Results: Over an 8-month period, C-CT significantly reduced relapse estimates more than control (10% vs 31%). Over 24 months, including the CT-free follow-up, age of onset and quality of remission during the late phase of A-CT each interacted with condition assignment to influence durability of effects. In patients with early-onset MDD, C-CT significantly reduced relapse and recurrence estimates (16% vs 67% in control). When patients had unstable remission during late A-CT, C-CT significantly reduced relapse and recurrence estimates to 37% (vs 62% in control).
Conclusions: Findings suggest that 8 months of C-CT significantly reduces relapse and recurrence in the highest-risk patients with recurrent MDD. Risk factors influenced the necessity for C-CT.
Figures
References
-
- Frank E, Kupfer DJ, Perel JM, Cornes C, Jarrett RB, Mallinger AG, Thase ME, McEachran AB, Grochocinski VJ. Three-year outcomes for maintenance therapies in recurrent depression. Arch Gen Psychiatry. 1990;47:1093–1099. - PubMed
-
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy of Depression. Guilford Press; New York, NY: 1979.
-
- Jarrett RB, Basco MR, Risser RC, Ramanan J, Marwill M, Kraft D, Rush AJ. Is there a role for continuation phase cognitive therapy for depressed outpatients? J Consult Clin Psychol. 1998;66:1036–1040. - PubMed
-
- Evans MD, Hollon SD, DeRubeis RJ, Piasecki JM, Grove WM, Garvey MJ, Tuason VB. Differential relapse following cognitive therapy and pharmacotherapy for depression. Arch Gen Psychiatry. 1992;49:802–808. - PubMed
-
- Kovacs M, Rush AJ, Beck AT, Hollon SD. Depressed outpatients treated with cognitive therapy or pharmacotherapy: a one-year follow-up. Arch Gen Psychiatry. 1981;38:33–39. - PubMed
