

Correlation of breath ammonia with blood urea nitrogen and creatinine during hemodialysis
- PMID: 11296293
- PMCID: PMC31883
- DOI: 10.1073/pnas.071057598
Correlation of breath ammonia with blood urea nitrogen and creatinine during hemodialysis
Abstract
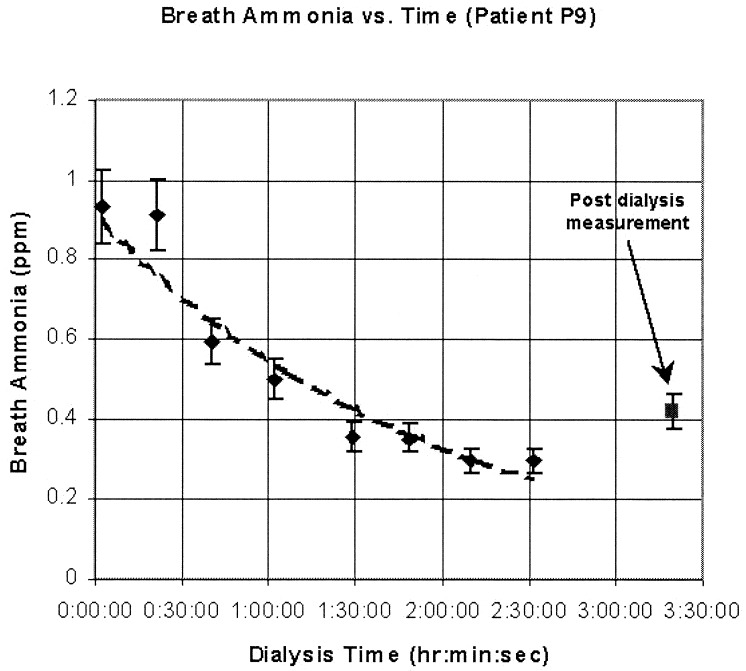
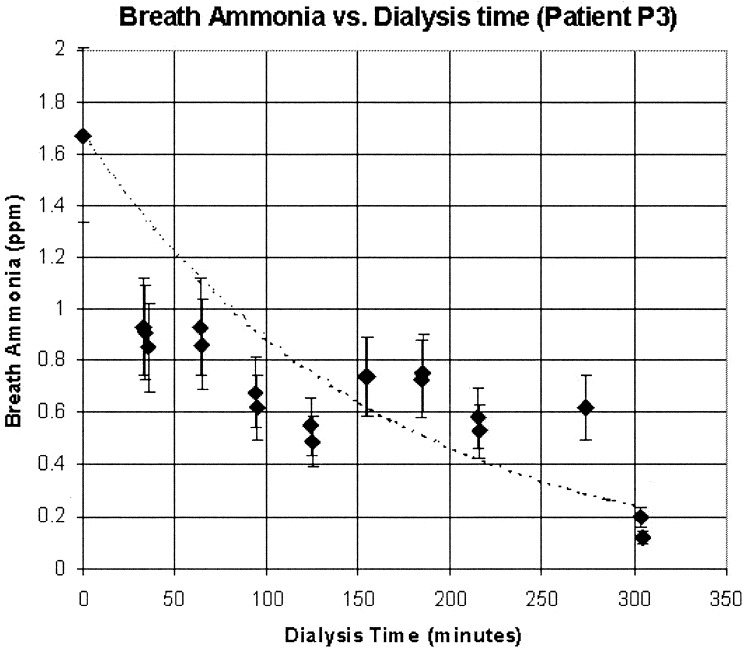
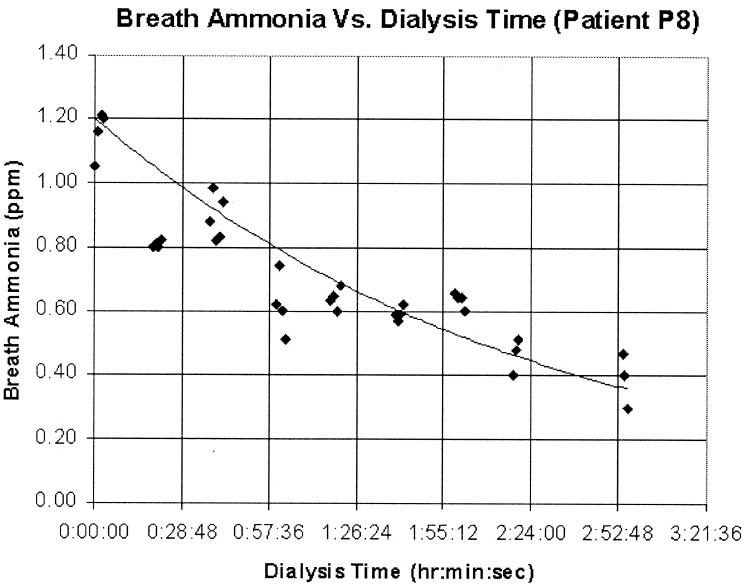
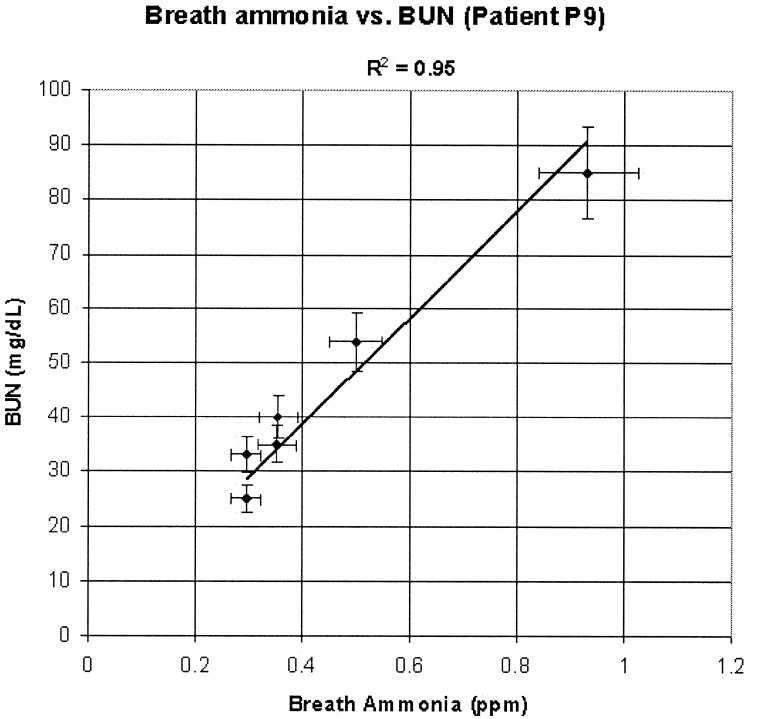
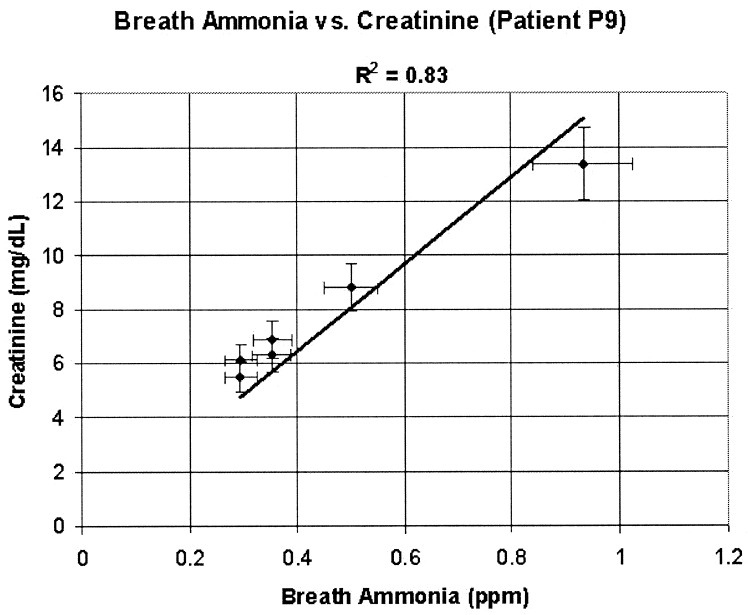
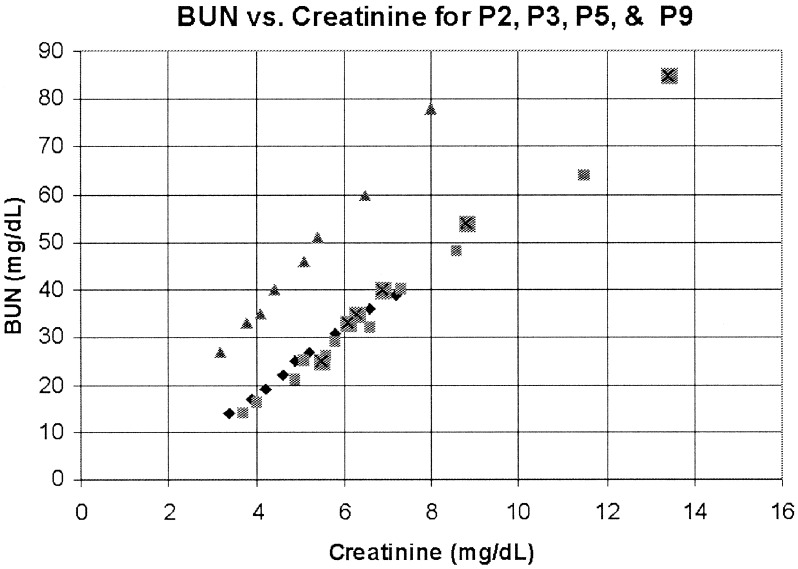
We have spectroscopically determined breath ammonia levels in seven patients with end-stage renal disease while they were undergoing hemodialysis at the University of California, Los Angeles, dialysis center. We correlated these measurements against simultaneously taken blood samples that were analyzed for blood urea nitrogen (BUN) and creatinine, which are the accepted standards indicating the level of nitrogenous waste loading in a patient's bloodstream. Initial levels of breath ammonia, i.e., at the beginning of dialysis, are between 1,500 ppb and 2,000 ppb (parts per billion). These levels drop very sharply in the first 15-30 min as the dialysis proceeds. We found the reduction in breath ammonia concentration to be relatively slow from this point on to the end of dialysis treatment, at which point the levels tapered off at 150 to 200 ppb. For each breath ammonia measurement, taken at 15-30 min intervals during the dialysis, we also sampled the patient's blood for BUN and creatinine. The breath ammonia data were available in real time, whereas the BUN and creatinine data were available generally 24 h later from the laboratory. We found a good correlation between breath ammonia concentration and BUN and creatinine. For one of the patients, the correlation gave an R(2) of 0.95 for breath ammonia and BUN correlation and an R(2) of 0.83 for breath ammonia and creatinine correlation. These preliminary data indicate the possibility of using the real-time breath ammonia measurements for determining efficacy and endpoint of hemodialysis.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
