

Functional results and visceral perception after ileo neo-rectal anastomosis in patients: a pilot study
- PMID: 11302969
- PMCID: PMC1728300
- DOI: 10.1136/gut.48.5.683
Functional results and visceral perception after ileo neo-rectal anastomosis in patients: a pilot study
Abstract
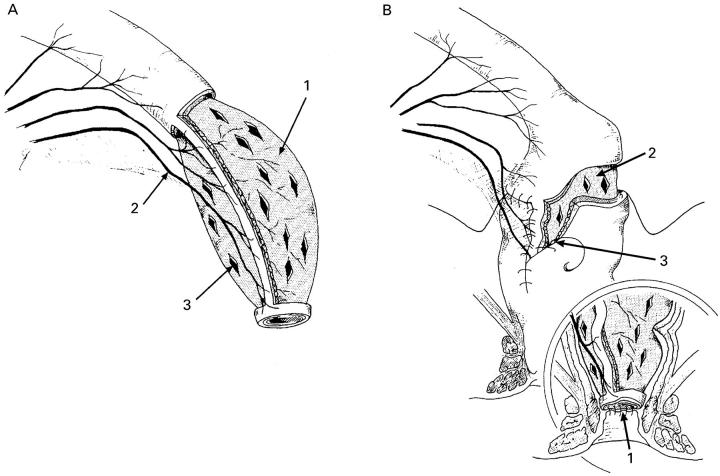
Introduction: To reduce pouch related complications after restorative proctocolectomy, an alternative procedure was developed, the ileo neo-rectal anastomosis (INRA). This technique consists of rectal mucosa replacement by ileal mucosa and straight ileorectal anastomosis. Our study provides a detailed description of the functional results after INRA.
Patients and methods: Eleven patients underwent an INRA procedure with a temporary ileostomy. Anorectal function tests were performed two months prior to and six and 12 months after closure of the ileostomy and comprised: anal manometry, ultrasound examination, rectal balloon distension, and transmucosal electrical nerve stimulation (TENS). Function was subsequently related to the histopathology of rectal biopsy samples.
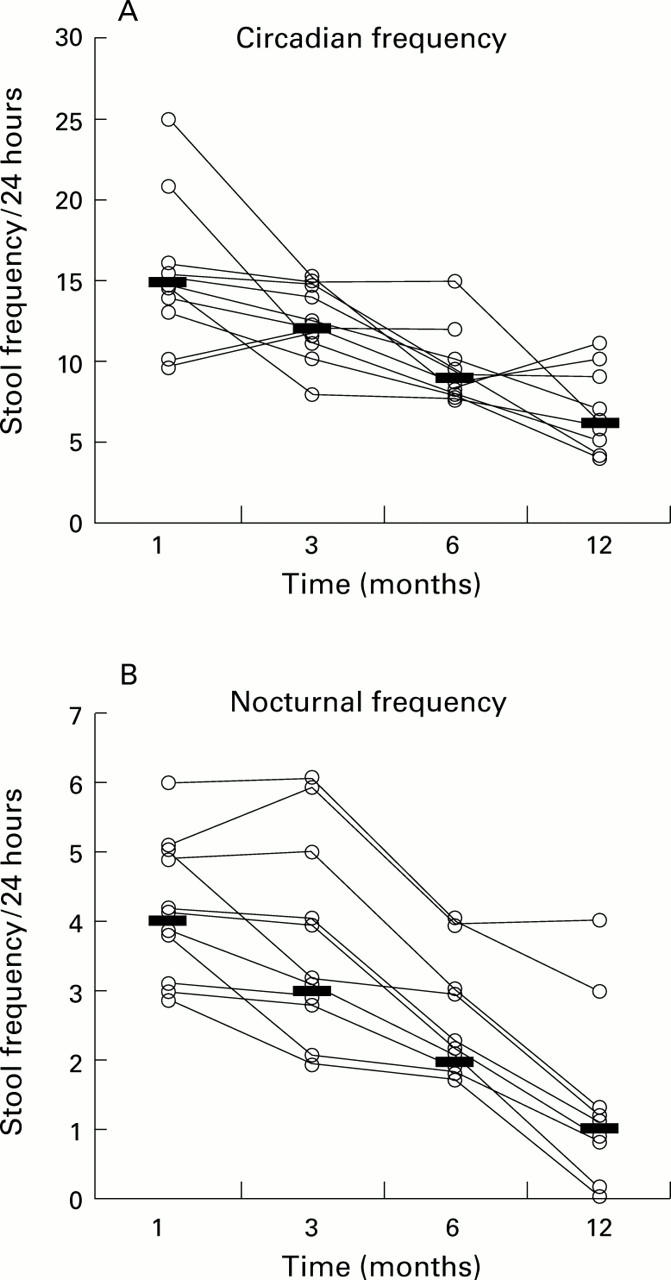
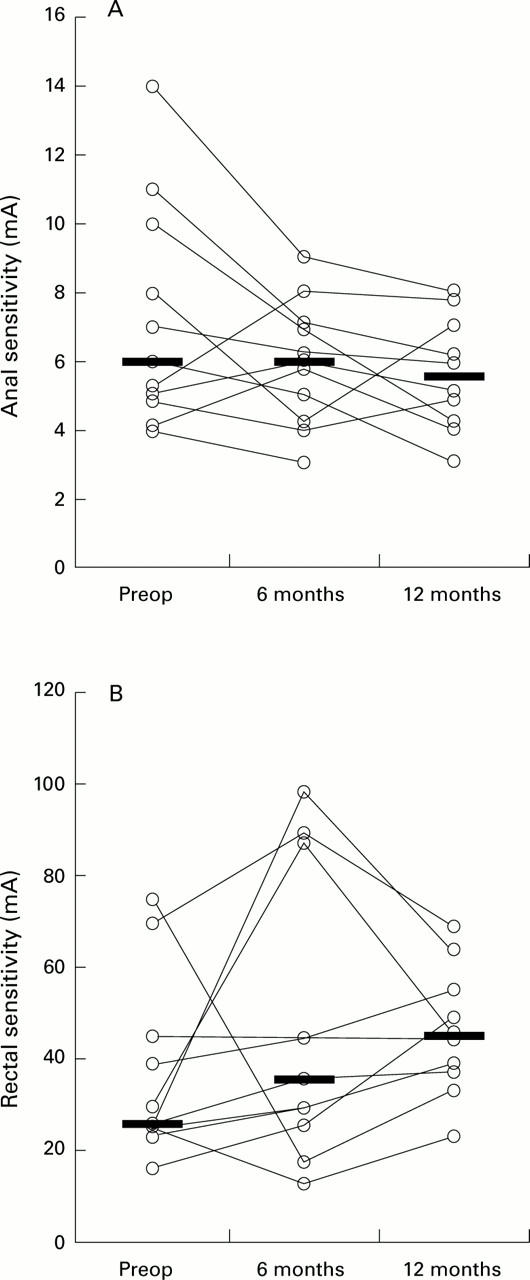
Results: Median stool frequency decreased from 15/24 hours (10-25) to 6/24 hours (4-11) at one year. All patients reported full continence. Anal sensibility, and resting and squeeze pressures did not change after INRA. Rectal compliance decreased (2.1 (0.7-2.8) v 1.5 (0.4-2.2) and 1.4 (0.8-3.7) ml/mm Hg (p=0.03)) but the maximum tolerated volume increased (70 (50-118) v 96 (39-176) (NS) and 122 (56-185) ml (p=0.03)). Decreasing rectal sensitivity was found: the maximum tolerated pressure increased (14 (8-24) v 22 (8-34) (NS) and 26 (14-40) (p=0.02)) and the rectal threshold for TENS displayed a similar tendency. All patients displayed a low grade chronic inflammatory infiltrate in neorectal biopsy samples before closure of the ileostomy, with no change during follow up.
Conclusions: The technique of INRA provides a safe alternative for restorative surgery. Stool frequency after INRA improves with time and seems to be related to decreasing sensitivity and not to histopathological changes in the neorectum. Furthermore, after the INRA procedure, all patients reported full continence.
Figures
Comment in
-
New pouches for old?Gut. 2001 May;48(5):592-3. doi: 10.1136/gut.48.5.592. Gut. 2001. PMID: 11302951 Free PMC article. No abstract available.
Similar articles
-
The ileo neo rectal anastomosis: long-term results of surgical innovation in patients after ulcerative colitis and familial adenomatous polyposis.Int J Colorectal Dis. 2013 Jan;28(1):111-8. doi: 10.1007/s00384-012-1545-0. Epub 2012 Aug 12. Int J Colorectal Dis. 2013. PMID: 22885881 Clinical Trial.
-
Ileoneorectal anastomosis: early clinical results of a restorative procedure for ulcerative colitis and familial adenomatous polyposis without formation of an ileoanal pouch.Ann Surg. 1999 Dec;230(6):750-7; discussion 757-8. doi: 10.1097/00000658-199912000-00003. Ann Surg. 1999. PMID: 10615929 Free PMC article.
-
Ileo-neorectal anastomosis: medium- and long-term follow-up of 37 patients.Dig Surg. 2004;21(5-6):371-8; discussion 379. doi: 10.1159/000081679. Epub 2004 Oct 20. Dig Surg. 2004. PMID: 15499222
-
[Technique and results of the ileoanal pouch after proctocolectomy].Zentralbl Chir. 1994;119(12):867-77. Zentralbl Chir. 1994. PMID: 7846969 Review. German.
-
Quest for continence: surgery for ulcerative colitis and familial adenomatous polyposis.Br J Hosp Med. 1994 Feb 2-15;51(3):108-110. Br J Hosp Med. 1994. PMID: 8193832 Review.
Cited by
-
The ileo neo rectal anastomosis: long-term results of surgical innovation in patients after ulcerative colitis and familial adenomatous polyposis.Int J Colorectal Dis. 2013 Jan;28(1):111-8. doi: 10.1007/s00384-012-1545-0. Epub 2012 Aug 12. Int J Colorectal Dis. 2013. PMID: 22885881 Clinical Trial.
-
Gastrointestinal motility disorders in inflammatory bowel diseases.World J Gastroenterol. 2014 Jan 7;20(1):37-44. doi: 10.3748/wjg.v20.i1.37. World J Gastroenterol. 2014. PMID: 24415856 Free PMC article. Review.
-
Evolution of the restorative proctocolectomy and its effects on gastrointestinal hormones.Int J Colorectal Dis. 2007 Oct;22(10):1143-63. doi: 10.1007/s00384-007-0331-x. Epub 2007 Jun 19. Int J Colorectal Dis. 2007. PMID: 17576578 Free PMC article. Review.
-
Sexual function and continence after ileo pouch anal anastomosis: a comparison between a meta-analysis and a questionnaire survey.Int J Colorectal Dis. 2004 May;19(3):215-8. doi: 10.1007/s00384-003-0543-7. Epub 2003 Oct 16. Int J Colorectal Dis. 2004. PMID: 14564464
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous