

Pulmonary preinvasive neoplasia
- PMID: 11304841
- PMCID: PMC1731391
- DOI: 10.1136/jcp.54.4.257
Pulmonary preinvasive neoplasia
Abstract
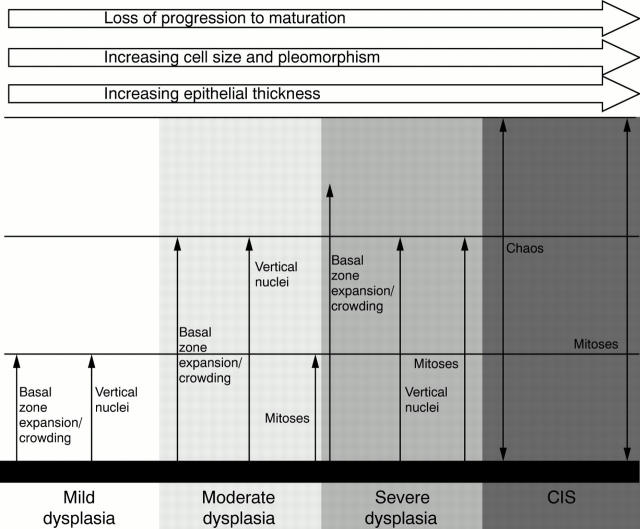
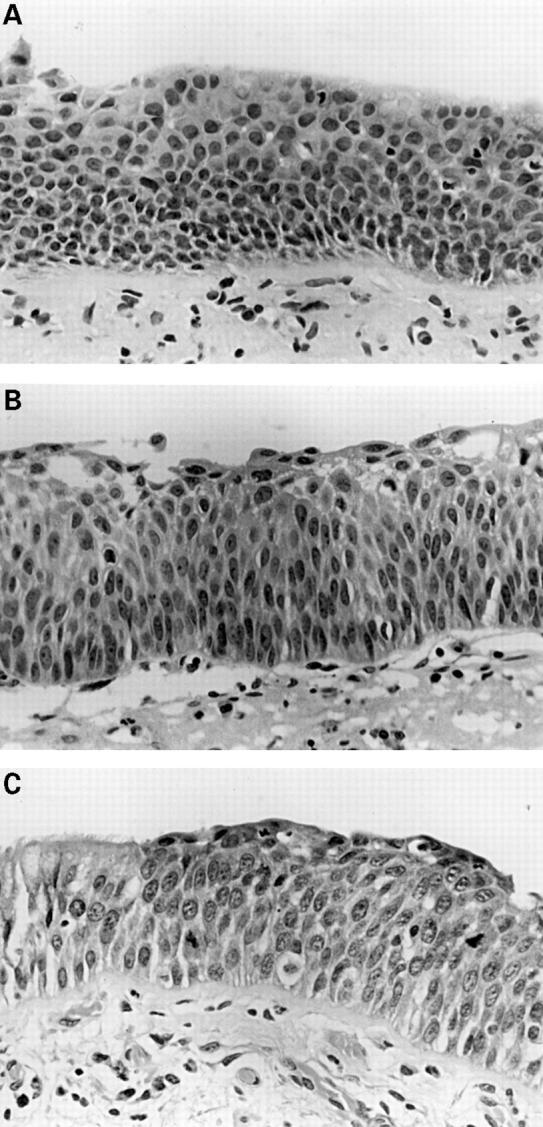
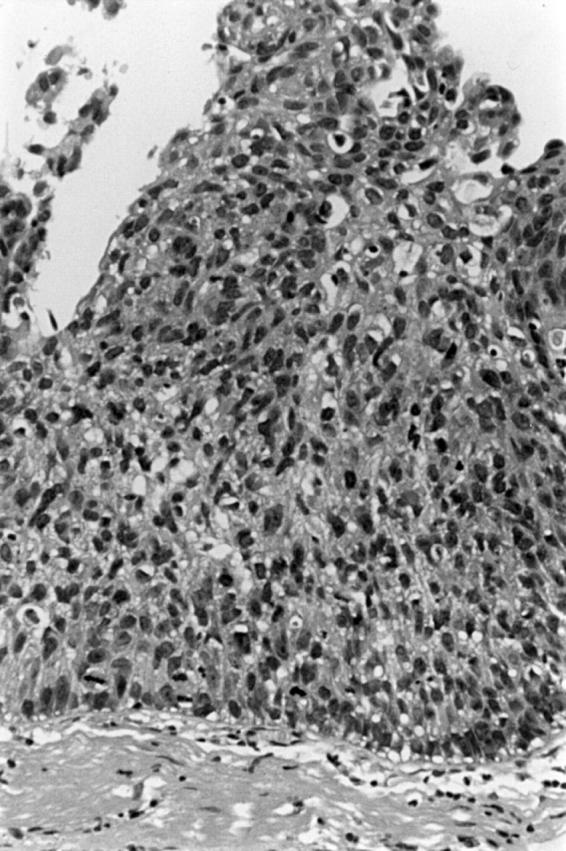
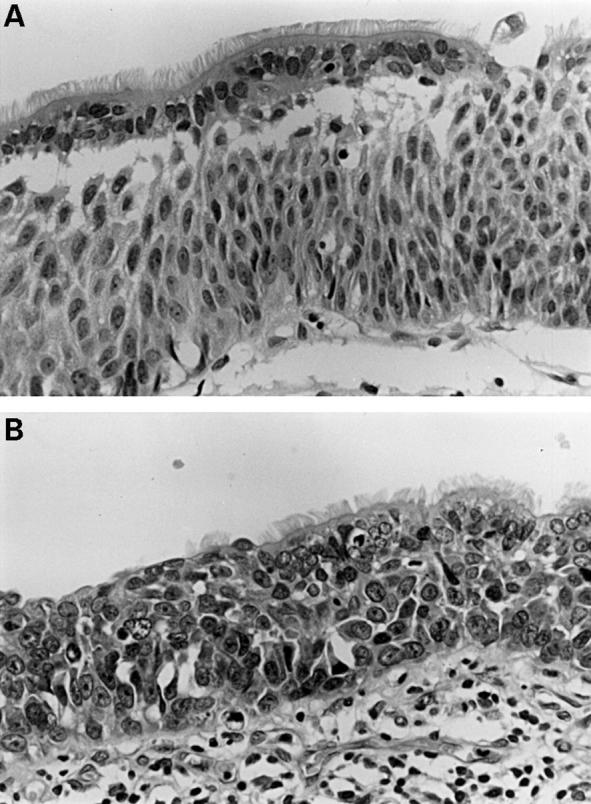
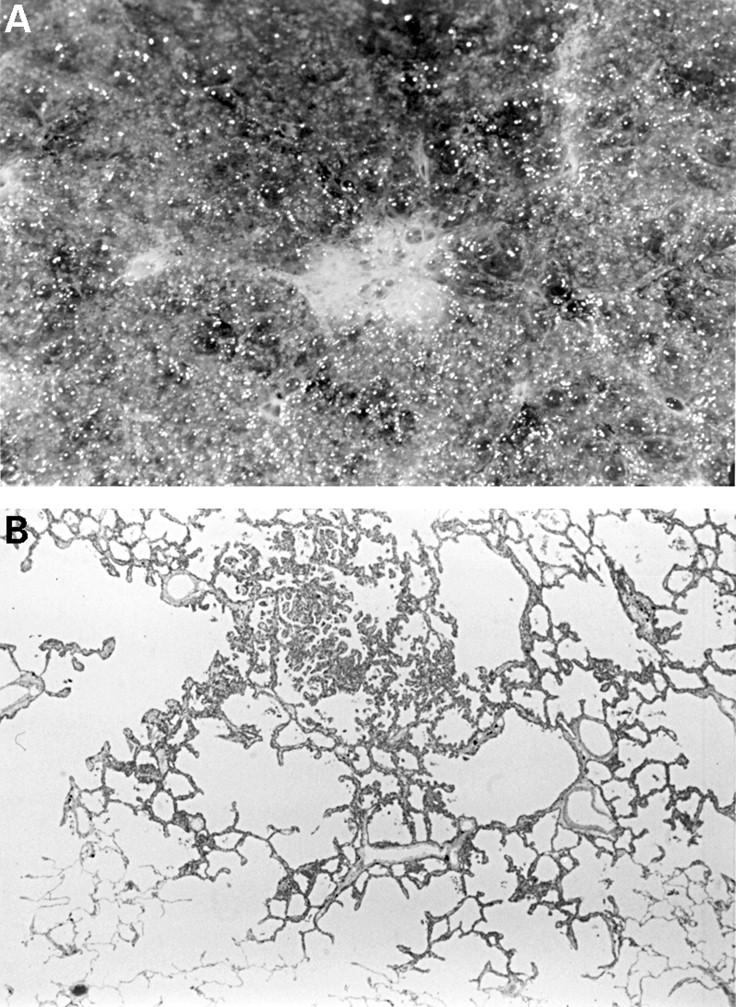
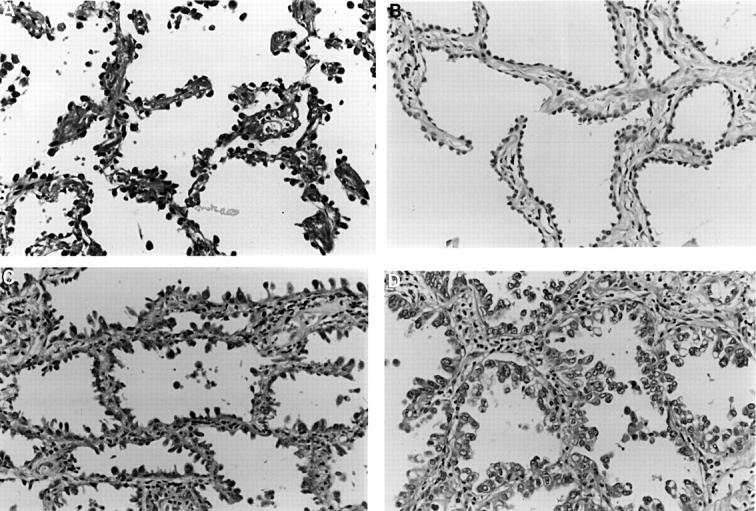
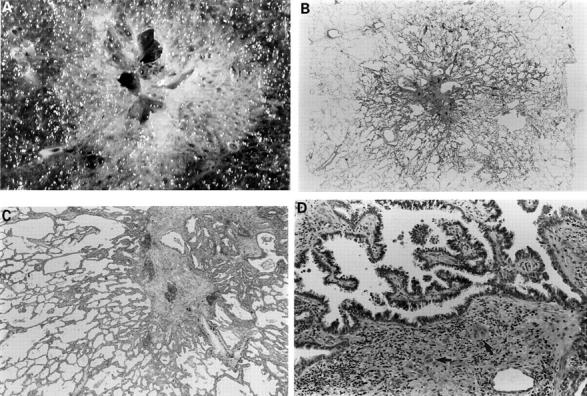
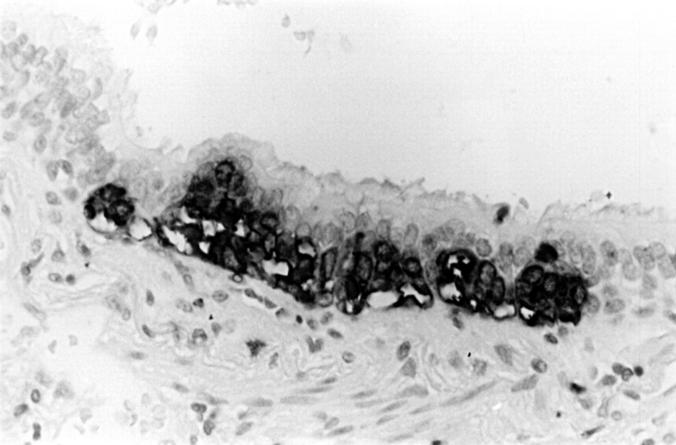
Advances in molecular biology have increased our knowledge of the biology of preneoplastic lesions in the human lung. The recently published WHO lung tumour classification defines three separate lesions that are regarded as preinvasive neoplasia. These are (1) squamous dysplasia and carcinoma in situ (SD/CIS), (2) atypical adenomatous hyperplasia (AAH), and (3) diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIP-NECH). SD/CIS is graded in four stages (mild, moderate, severe, and CIS), based upon the distribution of atypical cells and mitotic figures. Most airways showing SD/CIS demonstrate a range of grades; many epithelia are hard to assess and the reproducibility of this complex system remains to be established. Detailed criteria are, however, welcome and provide an objective framework on which to compare various molecular changes. Alterations in gene expression and chromosome structure known to be associated with malignant transformation can be demonstrated in CIS, less so in dysplasias, but also in morphologically normal epithelium. The changes might be sequential, and their frequency and number increase with atypia. Less is known of the "risk of progression" of SD/CIS to invasive "central" bronchial carcinoma. It may take between one and 10 years for invasion to occur, yet the lesion(s) may be reversible if carcinogen exposure ceases. AAH may be an important precursor lesion for peripheral "parenchymal" adenocarcinoma of the lung: the "adenoma" in an adenoma-carcinoma sequence. There is good morphological evidence that AAH may progress from low to high grade to bronchioloalveolar carcinoma (BAC; a non-invasive lesion by definition). Invasion then develops within BAC and peripheral lung adenocarcinoma evolves. The molecular events associated with this progression are not well understood and studies are hampered by a lack of clear criteria to distinguish high grade AAH from BAC. Nonetheless, as with SD/CIS, the patterns of expression of tumour associated genes are consistent with neoplastic progression. We have little idea of the incidence of AAH in the normal or "smoking" populations. It is found more frequently in cancer bearing lungs, especially in those with adenocarcinoma, and is more common in women. No data are available on the risk of progression of AAH. DIPNECH is an exceptionally rare lesion associated with the development of multiple carcinoid tumours. Almost nothing is known of its biology. Knowledge of these lesions will be crucial in the design and understanding of lung cancer screening programmes, where it is likely that the morphological and, more importantly perhaps, the molecular characteristics of these lesions will provide useful targets for detection and possibly even treatment.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical