

Physical fitness and activity as separate heart disease risk factors: a meta-analysis
- PMID: 11323544
- PMCID: PMC2821586
- DOI: 10.1097/00005768-200105000-00012
Physical fitness and activity as separate heart disease risk factors: a meta-analysis
Abstract
Objective: Public health policies for physical activity presume that the greatest health benefits are achieved by increasing physical activity among the least active. This presumption is based largely on studies of cardiorespiratory fitness. To assess whether studies of cardiorespiratory fitness are germane to physical activity guidelines, we compared the dose-response relationships between cardiovascular disease endpoints with leisure-time physical activity and fitness from published studies.
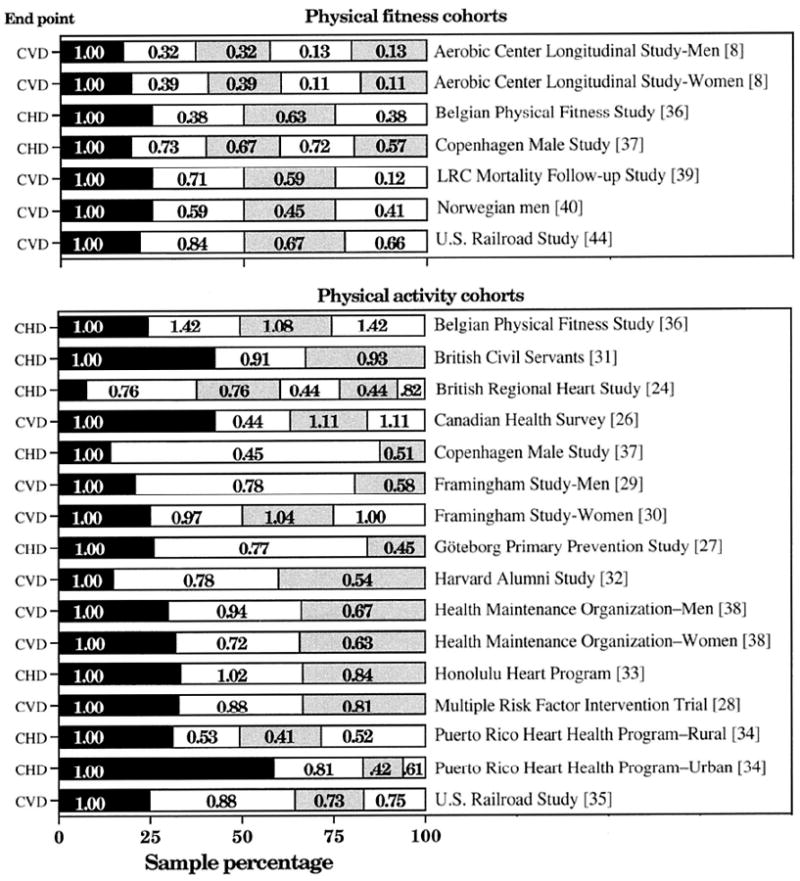
Data sources: Twenty-three sex-specific cohorts of physical activity or fitness (representing 1,325,004 person-years of follow-up), cited in Tables 4-1 and 4-2 of the Surgeon General's Report.
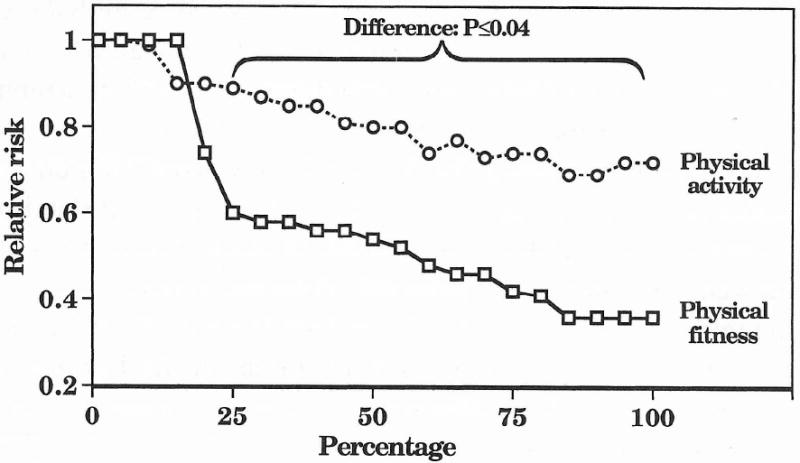
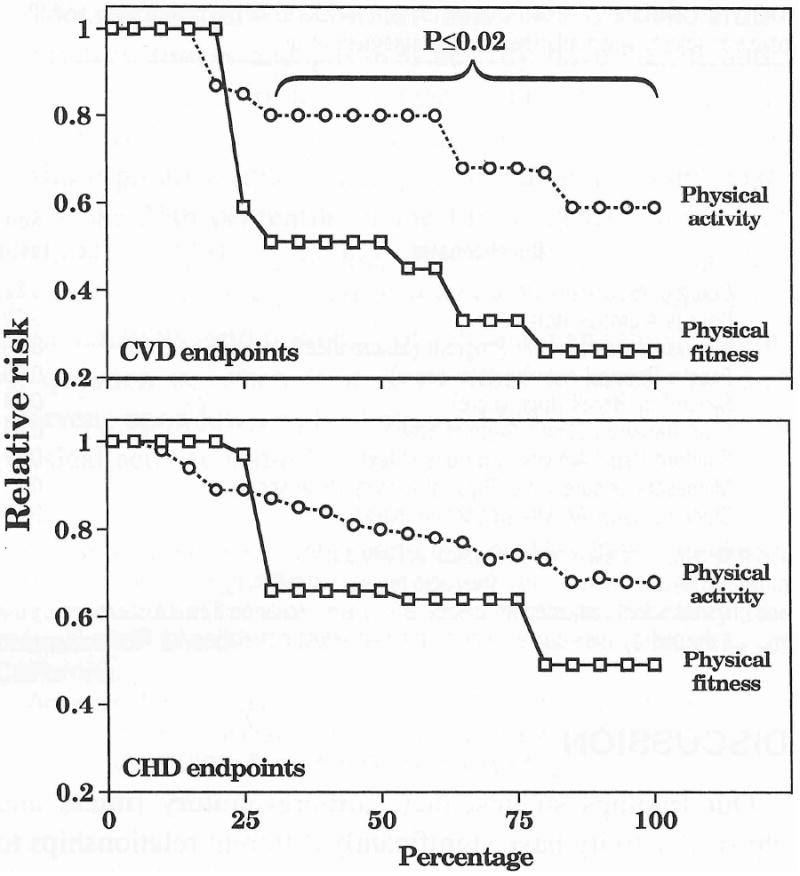
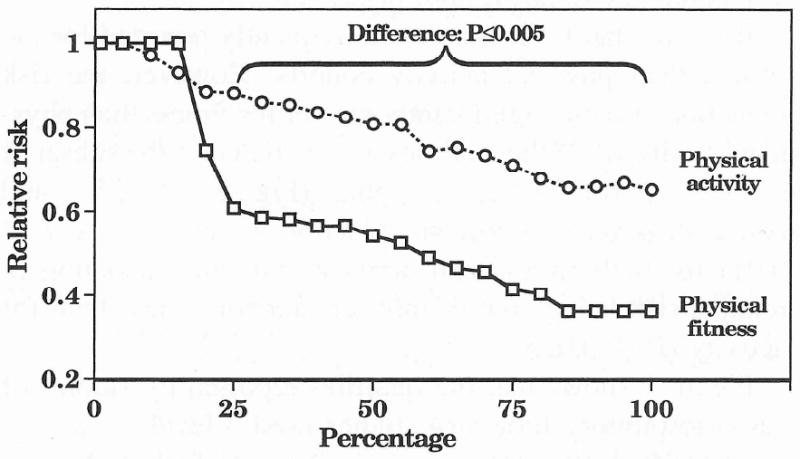
Data synthesis: Relative risks were plotted as a function of the cumulative percentages of the samples when ranked from least fit or active, to most fit or active. To combine study results, a weighted average of the relative risks over the 16 physical activity or seven fitness cohorts was computed at every 5th percentile between 5 and 100%. The analyses show that the risks of coronary heart disease or cardiovascular disease decrease linearly in association with increasing percentiles of physical activity. In contrast, there is a precipitous drop in risk occurring before the 25th percentile of the fitness distribution. As a consequence of this drop, there is a significant difference in the risk reduction associated with being more physically active or physically fit (P < or = 0.04).
Conclusions: Being unfit warrants consideration as a risk factor, distinctly from inactivity, and worthy of screening and intervention. Formulating physical activity recommendations on the basis of fitness studies may inappropriately demote the status of physical fitness as a risk factor while exaggerating the public health benefits of moderate amounts of physical activity.
Figures
Comment in
-
Physical fitness and activity as separate heart disease risk factors: a meta-analysis.Med Sci Sports Exerc. 2001 May;33(5):762-4. doi: 10.1097/00005768-200105000-00013. Med Sci Sports Exerc. 2001. PMID: 11323545 No abstract available.
References
-
- Arraiz GA, Wiggle DT, Mao Y. Risk assessment of physical activity and physical fitness in the Canada Health Survey mortality follow-up study. J Clin Epidemiol. 1992;45:419–428. - PubMed
-
- Bijnen FC, Caspersen CJ, Feskens EJ, et al. Physical activity and 10-year mortality from cardiovascular diseases and all causes: the Zutphen Elderly Study. Arch Intern Med. 1998;27:1499–1505. - PubMed
-
- Blair SN, Kohl HW, II, Barlow CE, et al. Changes in physical fitness and all-cause mortality: a prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–1098. - PubMed
-
- Blair SN, Kohl HW, III, Paffenbarger RS, Jr, et al. Physical fitness and all-cause mortality: a prospective study of healthy men and women. JAMA. 1989;262:2395–2401. - PubMed
-
- Bouchard C, Daw EW, Rice T, et al. Familial resemblance for VO2max in the sedentary state: the HERITAGE family study. Med Sci Sports Exerc. 1998;30:252–258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
