

Breast cancer survival by teaching status of the initial treating hospital
- PMID: 11332310
- PMCID: PMC80677
Breast cancer survival by teaching status of the initial treating hospital
Erratum in
- CMAJ 2001 May 1;164(9):1280
Abstract
Background: A number of studies have documented variation in treatment patterns by treatment setting or by region. In order to better understand how treatment setting might affect survival, we compared the survival outcomes of women with node-negative breast cancer who were initially treated at teaching hospitals with those of women initially treated at community hospitals.
Methods: We constructed a retrospective cohort consisting of a random sample of 938 cases, initially diagnosed in 1991, drawn from the Ontario Cancer Registry. Exposure was defined by the type of hospital in which the initial breast cancer surgery was performed. Outcomes were ascertained through follow-up of vital statistics.
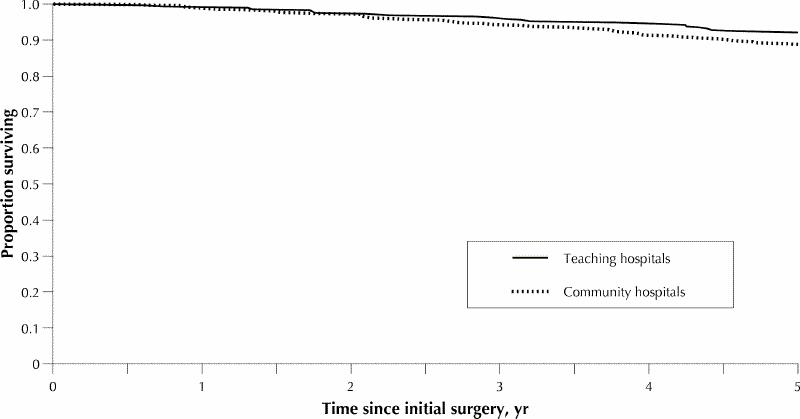
Results: The crude 5-year survival rate was 88.7% for women who had their initial surgery in a community hospital and 92.5% for women who had their initial surgery in a teaching hospital. Women in higher income neighbourhoods experienced better survival at 5 years regardless of which type of hospital they were treated in. Multivariate proportional hazards regression modelling demonstrated a 53% relative reduction in risk of death among women with tumours less than or equal to 20 mm in diameter who were treated at a teaching hospital (relative risk [RR] = 0.47, 95% confidence interval [CI] 0.23-0.96), whereas among those with larger tumours there was no demonstrated difference in survival (RR = 1.32, 95% CI 0.73-2.32). Other variables that were significant in the model were age at diagnosis, estrogen receptor status and the use of radiation therapy.
Interpretation: Women with node-negative breast cancer and tumours less than or equal to 20 mm in diameter who were initially seen at a teaching hospital had significantly better survival than women with similar tumours who were initially seen at a community hospital. Survival among women with larger tumours was not statistically significantly different for the 2 types of hospital.
Figures
Comment in
-
Specialization and cancer: words with too many meanings should be handled with care.CMAJ. 2001 Jan 23;164(2):210-1. CMAJ. 2001. PMID: 11332315 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):147, 149. CMAJ. 2001. PMID: 11501445 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):147; author reply 149, 151. CMAJ. 2001. PMID: 11501446 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):147; author reply 149, 151. CMAJ. 2001. PMID: 11501447 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):149; author reply 149, 151. CMAJ. 2001. PMID: 11501448 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):149; author reply 149, 151. CMAJ. 2001. PMID: 11501449 Free PMC article. No abstract available.
-
Do women treated for breast cancer at teaching hospitals really fare better?CMAJ. 2001 Jul 24;165(2):149; author reply 149, 151. CMAJ. 2001. PMID: 11501450 Free PMC article. No abstract available.
Similar articles
-
Influence of hospital characteristics on operative death and survival of patients after major cancer surgery in Ontario.Can J Surg. 2006 Aug;49(4):251-8. Can J Surg. 2006. PMID: 16948883 Free PMC article.
-
Investigating the correlation between hospital of primary treatment and the survival of women with breast cancer.Cancer. 2005 Oct 1;104(7):1343-8. doi: 10.1002/cncr.21336. Cancer. 2005. PMID: 16080144
-
Are many community hospitals undertreating breast cancer?: lessons from 24,834 patients.Ann Surg. 2008 Aug;248(2):154-62. doi: 10.1097/SLA.0b013e31816c4030. Ann Surg. 2008. PMID: 18650623
-
Treatment differences and other prognostic factors related to breast cancer survival. Delivery systems and medical outcomes.JAMA. 1994 Apr 20;271(15):1163-8. JAMA. 1994. PMID: 8151873
-
RECPAM analysis of prognostic factors in patients with stage III breast cancer.Breast Cancer Res Treat. 1990 Oct;16(3):231-42. doi: 10.1007/BF01806331. Breast Cancer Res Treat. 1990. PMID: 2085674 Review.
Cited by
-
Effects of payer status on breast cancer survival: a retrospective study.BMC Cancer. 2015 Apr 1;15:211. doi: 10.1186/s12885-015-1228-7. BMC Cancer. 2015. PMID: 25884399 Free PMC article.
-
Technical factors, surgeon case volume and positive margin rates after breast conservation surgery for early-stage breast cancer.Can J Surg. 2010 Oct;53(5):305-12. Can J Surg. 2010. PMID: 20858374 Free PMC article.
-
Surgeon Factors Influencing Breast Surgery Outcomes: A Scoping Review to Define the Modern Breast Surgical Oncologist.Ann Surg Oncol. 2023 Aug;30(8):4695-4713. doi: 10.1245/s10434-023-13472-w. Epub 2023 Apr 10. Ann Surg Oncol. 2023. PMID: 37036590
-
Survival trends among non-small-cell lung cancer patients over a decade: impact of initial therapy at academic centers.Cancer Med. 2018 Oct;7(10):4932-4942. doi: 10.1002/cam4.1749. Epub 2018 Sep 2. Cancer Med. 2018. PMID: 30175515 Free PMC article.
-
A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario.CMAJ. 2001 Aug 21;165(4):421-5. CMAJ. 2001. PMID: 11531050 Free PMC article.
References
-
- Goel V, Olivotto I, Hislop TG, Sawka C, Coldman A, Holowaty EJ. Patterns of initial management of node-negative breast cancer in two Canadian provinces. CMAJ 1997;156(1):25-35. Abstract available: www.cma.ca/cmaj/vol-156/issue-1/0025.htm - PMC - PubMed
-
- Palda VA, Goel V, Sawka CA. The rise of tamoxifen: temporal and geographical trends of tamoxifen use in Ontario. Breast Cancer Res Treat 1997;43:33-41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical