

Case Reports
Mycotic aneurysm and cerebral infarction resulting from fungal sinusitis: imaging and pathologic correlation
Affiliations
- PMID: 11337328
- PMCID: PMC8174942
Item in Clipboard
Case Reports
Mycotic aneurysm and cerebral infarction resulting from fungal sinusitis: imaging and pathologic correlation
AJNR Am J Neuroradiol.
2001 May.
Abstract
A 73-year-old man was admitted with invasive aspergillus of the sphenoid sinus. Endoscopic debridement of the sphenoid sinus was complicated by rupture of a mycotic cavernous carotid artery aneurysm with severe epistaxis. The aneurysm was closed emergently by endovascular coil placement. Subsequently, the mycotic aneurysm extended intradurally and caused fatal subarachnoid hemorrhage. The radiologic-pathologic data illustrate the mechanism of fungal mycotic aneurysm formation and growth. This case emphasizes the need for rapid diagnosis of potential fungal involvement of the central nervous system and suggests the necessity for aggressive treatment once fungal cerebrovascular involvement is identified.
Figures
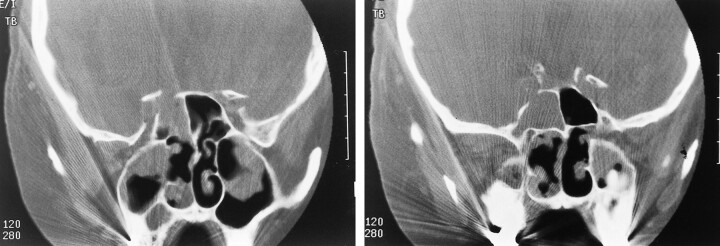
A and B, Coronal CT scan shows soft tissue density within the sphenoid sinus, with bony destruction in the region of the cavernous portion of the right internal carotid artery
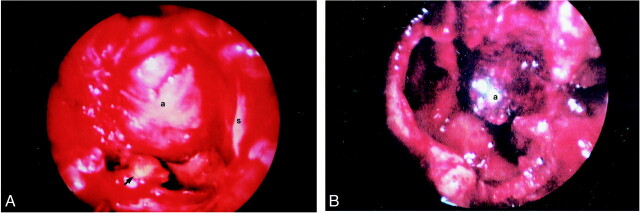
A, Endoscopic view of the sphenoid sinus following removal of the inspissated mucus and fungal debris. The most lateral and inferior portions of the sinus are evident (arrowhead). The aneurysm (a) projects from the superior aspect of the sphenoid, to nearly fill the sinus (s = midline nasal septum). B, Endoscopic view of the sphenoid sinus approximately 5 days after embolization. There is no evidence of recurrent fungal debris and the embolized aneurysm is much smaller
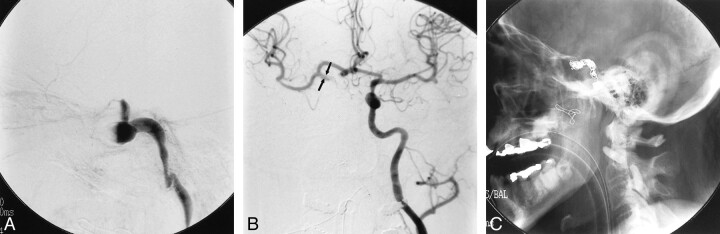
A, Lateral view, angiogram of the right internal carotid artery following initial debridement and packing of the sphenoid sinus shows fusiform dilation of the cavernous portion of the vessel. Occlusion of the carotid artery resulted from packing of the sphenoid sinus at the time of surgery. B, Injection of the left internal carotid artery shows good filling across the anterior communicating artery. The visualized portions of the supraclinoid right internal carotid artery (arrows) and the right middle cerebral artery are of normal caliber. C, Postembolization plain film shows microcoils within the lumen of the aneurysm and proximal detachable balloons occluding the right internal carotid artery
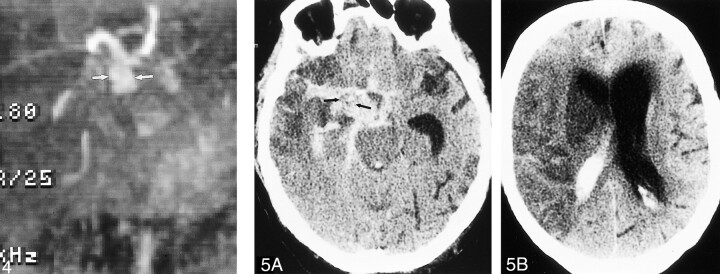
MR angiogram (time of flight, 48/5.9 [TR/TE]) shows dilated supraclinoid right internal carotid artery (arrows) representing aneurysmal progression from angiogram performed at the time of embolization. fig 5. A, Unenhanced CT scan shows extensive subarachnoid hemorrhage outlining soft tissue mass (arrows) in the right basilar cistern, which represents the supraclinoid portion of the aneurysm. B, Hypodense cerebral infarct with mass effect is present throughout the right middle cerebral artery distribution
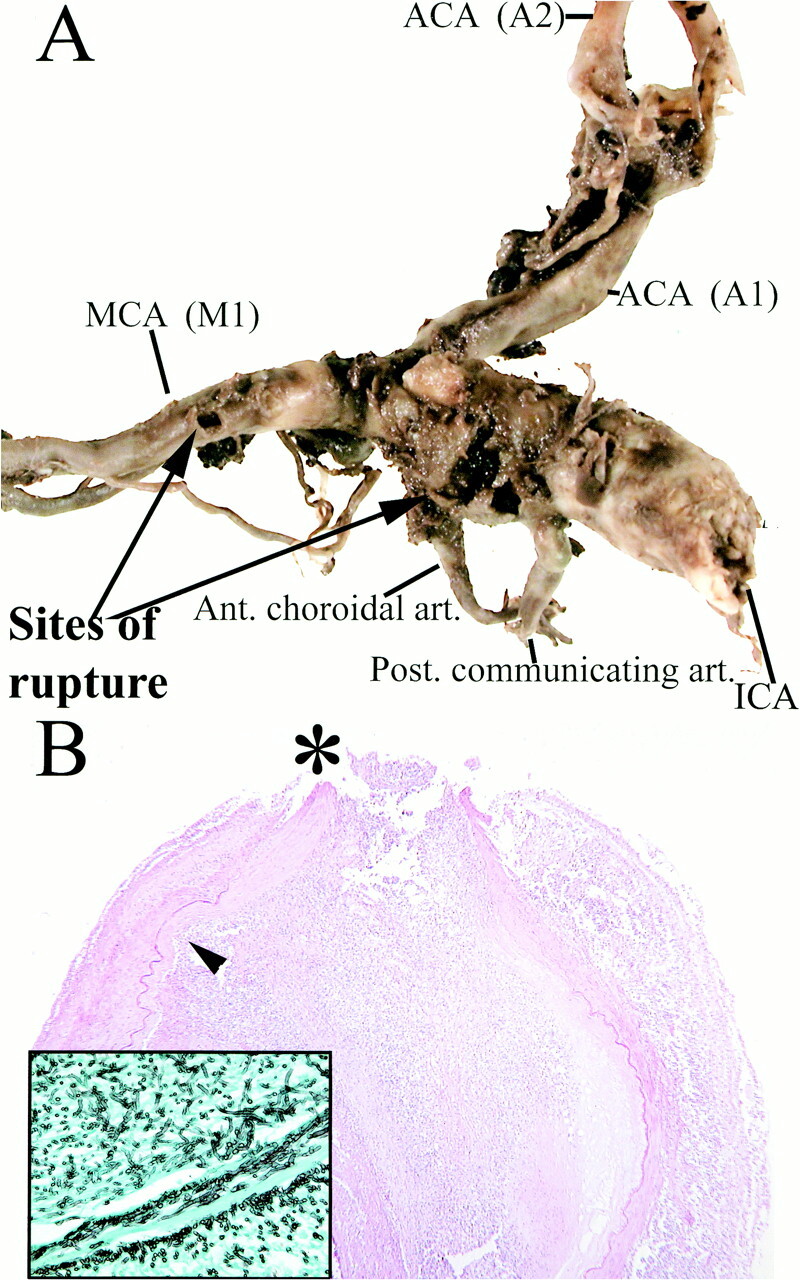
A, Aneurysmal dilation of the supraclinoid segment of the right internal carotid artery. Rupture sites (arrows) are present between the posterior communicating and anterior choroidal arteries, as well as along the M1 segment of the right middle cerebral artery. B, Histopathologic examination shows severe inflammatory change, necrosis of the arterial wall and elastica, intralumenal thrombosis, and focal rupture site (asterisk). Inset: (Grocott stain) Septated hyphae branching at acute angles, morphologically consistent with aspergillus species, located predominantely in the vessel wall and adventitia are seen
References
-
- Frazee J. Inflammatory aneurysms. In: Wilkins R, Rengachary S, eds. Neurosurgery. New York: McGraw Hill; 1996:2378–2382
-
- Mahaley M, Spock A. An ususual case of intracranial aneurysm. In: Smith J, ed. Neuro-Ophthalmology. St. Louis: Mosby; 1968:158–166
-
- Beal M, O'Carroll C, Kleinman G, Grossman R. Aspergillosis of the nervous system. Neurology 1982;32:473-479 - PubMed
-
- Sekhar L, Dujovny M, Rao G. Carotid-cavernous sinus thrombosis caused by aspergillus fumigatus. Case report. J Neurosurg 1980;52:120-125 - PubMed
-
- Takeshita M, Izawa M, Kubo O, et al. Aspergillotic aneurysm formation of cerebral artery following neurosurgical operation. Surg Neurol 1992;38:146-151 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical