

Case Reports
New advances in the management of acute coronary syndromes: 1. Matching treatment to risk
Affiliations
- PMID: 11341143
- PMCID: PMC81024
Item in Clipboard
Case Reports
New advances in the management of acute coronary syndromes: 1. Matching treatment to risk
CMAJ.
.
No abstract available
Figures
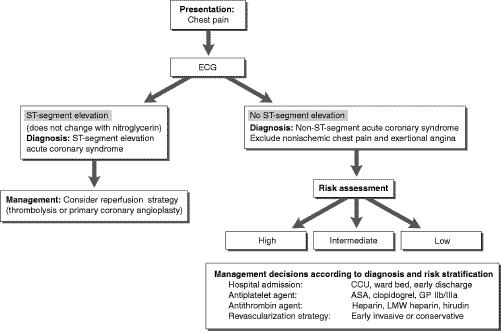
Fig. 1: Diagnostic triage and management of patients presenting to the emergency department with chest pain and a clinical suspicion of an acute coronary syndrome (unstable angina or myocardial infarction). CCU = coronary care unit, GP IIb/IIIa = glycoprotein IIb/IIIa inhibitor, LMW = low-molecular-weight. Photo by: Christine Kenney
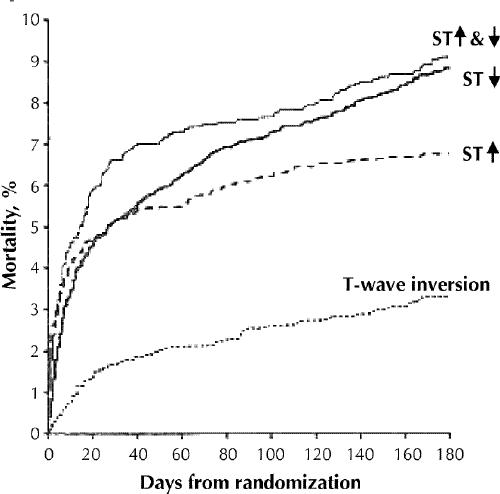
Fig. 2: Six-month mortality among patients with an acute coronary syndrome, by electrocardiogram result at time of presentation. Although patients with ST-segment depression (ST↓) have a better early (5-day) survival than those with ST-segment elevation (ST↑), their long-term outlook is as bad, if not worse. In this study patients at lowest risk were those with T-wave inversion alone. [Adapted, with permission, from Savonitto et al, JAMA 1999;281:707-13. Copyrighted 1999, American Medical Assocation.]
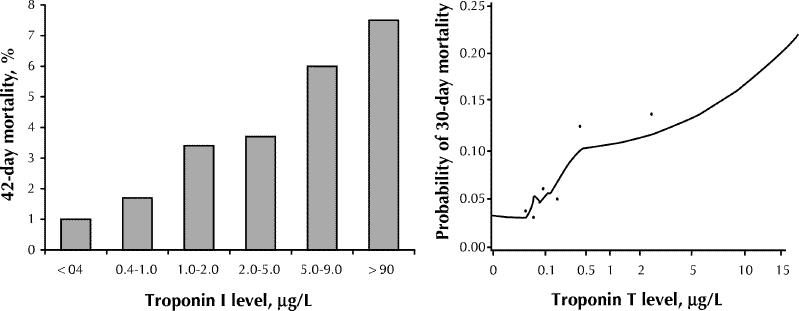
Fig. 3: Mortality in relation to cardiac troponin levels at time of randomization. Left: Troponin I, in TIMI IIIB study [adapted, with permission, from Antman et al, N Engl J Med 1996;335:1342-9]. Right: Troponin T, in GUSTO-IIa study [adapted, with permission, from Ohman et al, N Engl J Med 1996;335:1333-41].
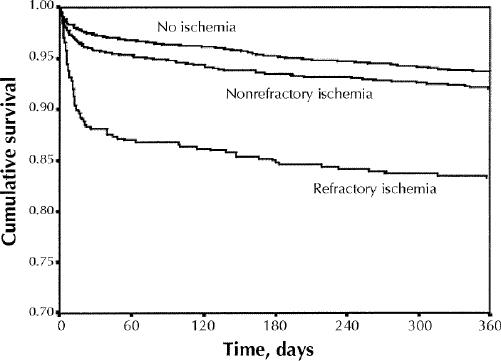
Fig. 4: Cumulative survival during the 360 days following acute coronary syndrome (ACS) with non-ST-segment elevation ACS in patients with refractory myocardial ischemia. [Adapted, with permission, from Armstrong et al, Circulation 1998;98:1860-8.]
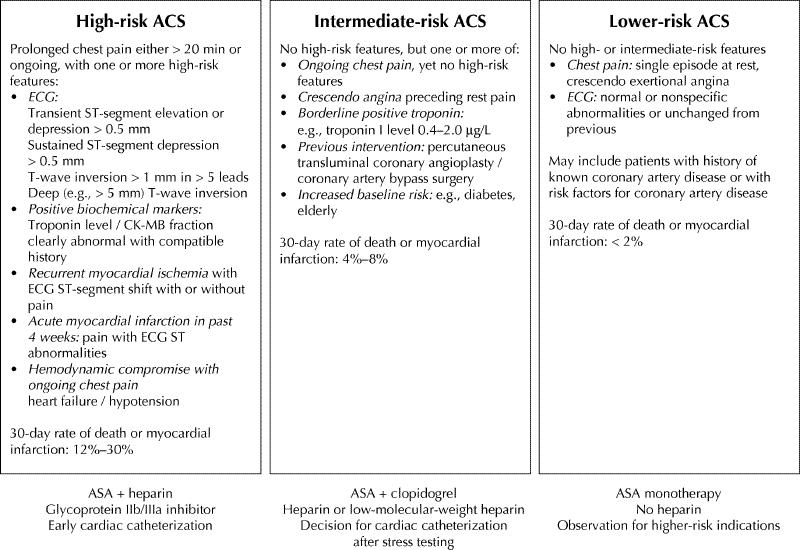
Fig. 5: Risk stratification of patients presenting with a non-ST-segment elevation acute coronary syndrome (ACS). Identification of high-, intermediate- and low-risk categories allows appropriate management choices. [Adapted, with permission, from Fitchett, Can J Cardiol 2000;16:1423-32.]
Comment in
-
New advances in the management of acute coronary syndromes.CMAJ. 2001 May 1;164(9):1303-4. CMAJ. 2001. PMID: 11341141 Free PMC article. No abstract available.
-
Evaluating the risks of therapies for acute coronary syndromes.CMAJ. 2001 Nov 13;165(10):1302-3. CMAJ. 2001. PMID: 11760974 Free PMC article. No abstract available.
-
Troponin assays for coronary syndrome diagnosis.CMAJ. 2002 Jan 8;166(1):13-4. CMAJ. 2002. PMID: 11800237 Free PMC article. No abstract available.
References
-
- Rahimtoola SH. Coronary bypass surgery for unstable angina. Circulation 1984; 69:842-8. - PubMed
-
- Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists' (FTT) Collaborative Group. Lancet 1994;343:311-22. - PubMed
-
- Rude RE, Poole WK, Muller JE, Turi Z, Rutherford J, Parker C, et al. Electrocardiographic and clinical criteria for the recognition of acute myocardial infarction based on analysis of 3,697 patients. Am J Cardiol 1983;52:936-42. - PubMed
-
- Margolis JR, Kannel WS, Feinleib M, Dawber TR, McNamara PM. Clinical features of unrecognized myocardial infarction — silent and symptomatic. Eighteen year follow-up: the Framingham study. Am J Cardiol 1973;32:1-7. - PubMed
-
- Kannel WB, Abbott RD. Incidence and prognosis of unrecognized myocardial infarction: an update on the Framingham study. N Engl J Med 1984;311:1144-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources