

Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects
- PMID: 11350851
- PMCID: PMC1753664
- DOI: 10.1136/ard.60.6.612
Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects
Abstract
Objectives: To investigate whether subjects with knee osteoarthritis (OA) have reduced static postural control, knee proprioceptive acuity, and maximal voluntary contraction (MVC) of the quadriceps compared with normal controls, and to determine possible independent predictors of static postural sway.
Methods: 77 subjects with symptomatic and radiographic knee OA (58 women, 19 men; mean age 63.4 years, range 36-82) and 63 controls with asymptomatic and clinically normal knees (45 women, 18 men; mean age 63 years, range 46-85) underwent assessment of static postural sway. 108 subjects (59 patients, 49 controls) also underwent assessment of knee proprioceptive activity and MVC (including calculation of quadriceps activation). In patients with knee OA knee pain, stiffness, and functional disability were assessed using the WOMAC Index. The height (m) and weight (kg) of all subjects was assessed.
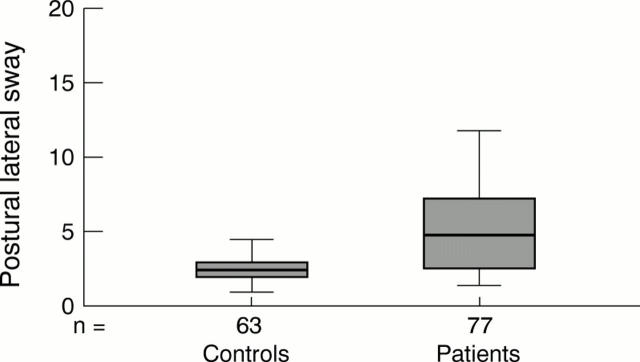
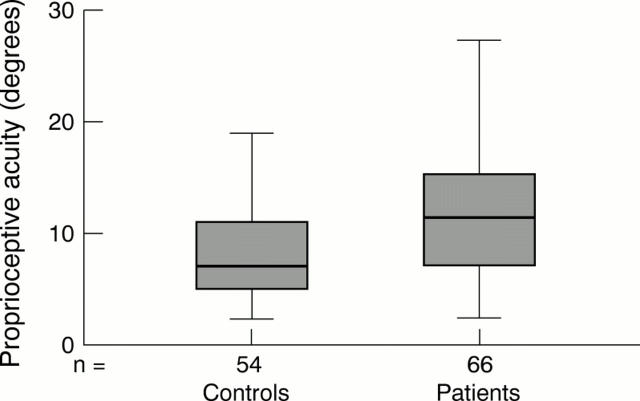
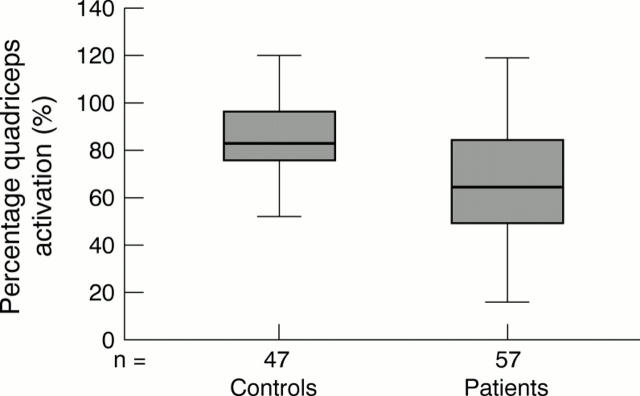
Results: Compared with controls, patients with knee OA were heavier (mean difference 15.3 kg, p<0.001), had increased postural lateral sway (controls: median 2.3, interquartile (IQ) range 1.8-2.9; patients: median 4.7, IQ range 1.9-4.7, p<0.001), reduced proprioceptive acuity (controls: mean 7.9, 95% CI 6.9 to 8.9; patients: mean 12.0, 95% CI 10.5 to 13.6, p<0.001), weaker quadriceps strength (controls: mean 22.5, 95% CI 19.9 to 24.6; patients: mean 14.7, 95% CI 12.5 to 16.9, p<0.001), and less percentage activation of quadriceps (controls: mean 87.4, 95% CI 80.7 to 94.2; patients: mean 66.0, 95% CI 58.8 to 73.2, p<0.001). The significant predictors of postural sway were knee pain and the ratio of MVC/body weight.
Conclusions: Compared with age and sex matched controls, subjects with symptomatic knee OA have quadriceps weakness, reduced knee proprioception, and increased postural sway. Pain and muscle strength may particularly influence postural sway. The interaction between physiological, structural, and functional abnormalities in knee OA deserves further study.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
