

Increase in mortality rates from intrahepatic cholangiocarcinoma in England and Wales 1968-1998
- PMID: 11358902
- PMCID: PMC1728314
- DOI: 10.1136/gut.48.6.816
Increase in mortality rates from intrahepatic cholangiocarcinoma in England and Wales 1968-1998
Erratum in
- Gut 2001 Aug;49(2):315
Abstract
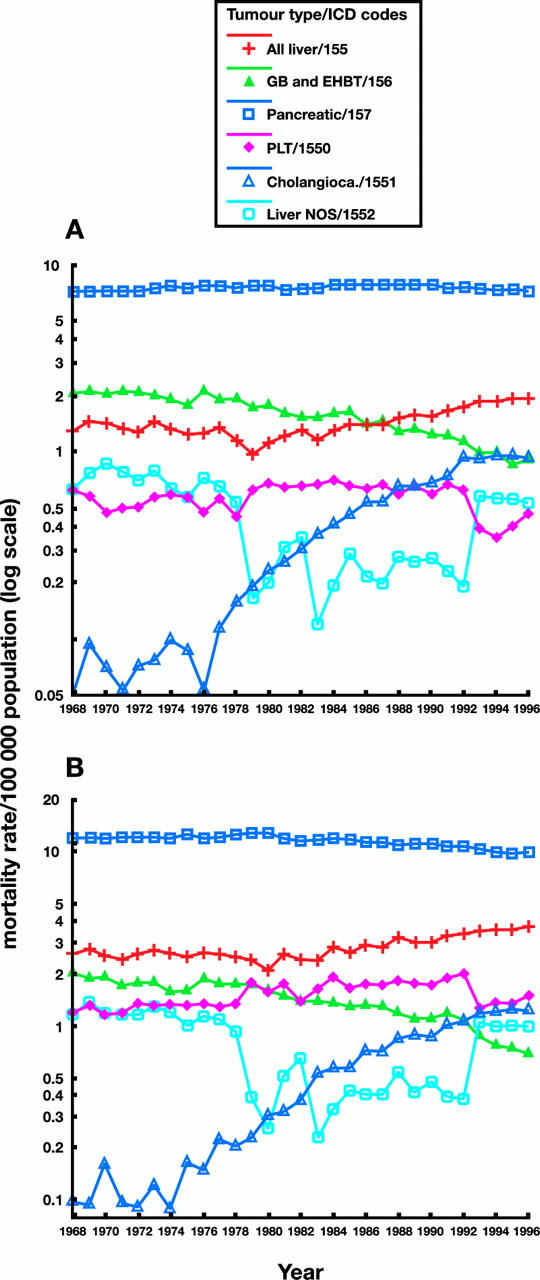
Background: The age standardised mortality rate per 100 000 population for all causes of liver tumours (International Classification of Disease 9 (ICD-9) 155) has almost doubled in England and Wales during the period 1979-1996. We further analysed the mortality statistics to determine which anatomical subcategories were involved.
Methods: Mortality statistics for liver tumours of ICD-9 155, 156, and subcategories, and for tumours of the pancreas (ICD-9 157), in England and Wales were investigated from the Office for National Statistics, London, from 1968 to 1996 inclusive. Data for 1997 and 1998 were also available on intrahepatic cholangiocarcinomas.
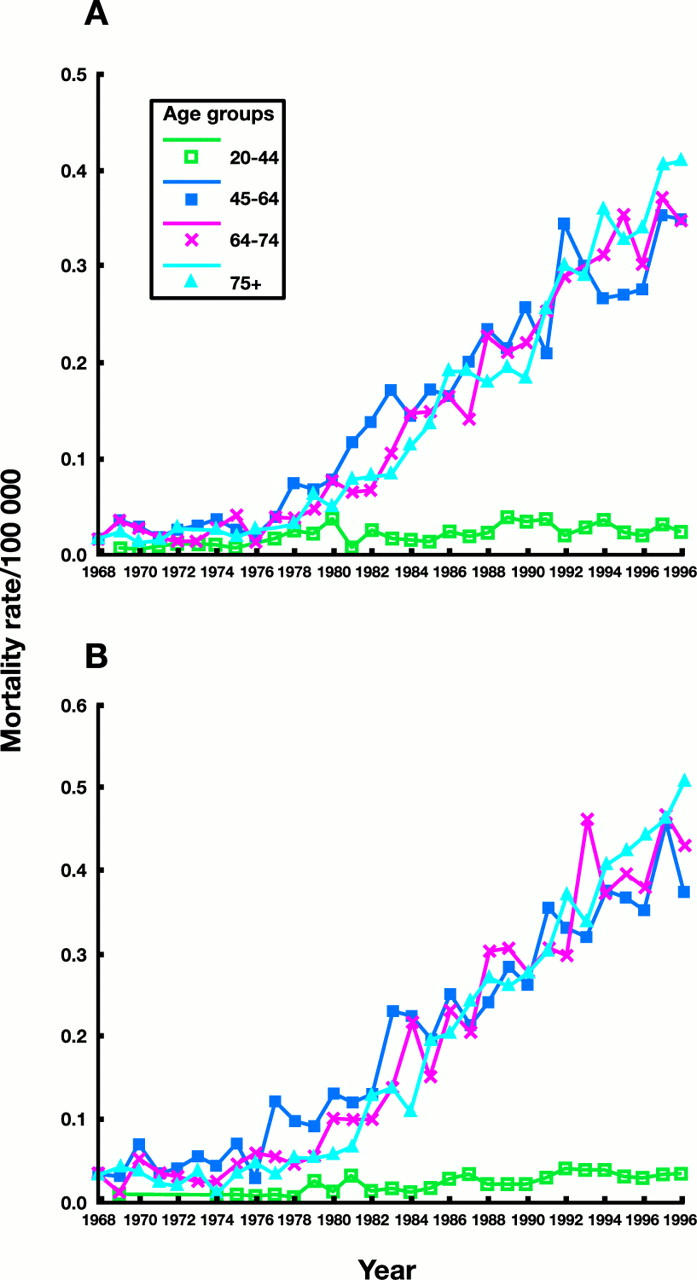
Results: There has been a marked rise in age standardised mortality rates for intrahepatic cholangiocarcinoma. Since 1993, it represents the commonest recorded cause of liver tumour related death in England and Wales. This is evident in age groups older than 45 years. In contrast, mortality trends from other primary liver tumours, including hepatocellular carcinoma, were unremarkable.
Conclusions: The observed increase in mortality from intrahepatic cholangiocarcinoma may represent better case ascertainment and diagnosis due to improved diagnostic imaging, use of image guided biopsies, or increased use of ERCP. However, the trend started before ERCP was introduced nationally, mortality rates have continued to increase steadily thereafter, and there is no clear evidence that diagnostic transfers easily explains the findings. Alternatively, these observations may represent a true increase in intrahepatic bile duct tumours. Epidemiological studies are required to determine whether there is any geographical clustering of cases around the UK.
Figures
Comment in
-
Small fry starting to make waves.Gut. 2001 Jun;48(6):754-5. doi: 10.1136/gut.48.6.754. Gut. 2001. PMID: 11358887 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical