

Review
doi: 10.1136/bjo.85.6.746.
Advanced glycation: an important pathological event in diabetic and age related ocular disease
Affiliations
- PMID: 11371498
- PMCID: PMC1723990
- DOI: 10.1136/bjo.85.6.746
Item in Clipboard
Review
Advanced glycation: an important pathological event in diabetic and age related ocular disease
Br J Ophthalmol.
2001 Jun.
No abstract available
Figures
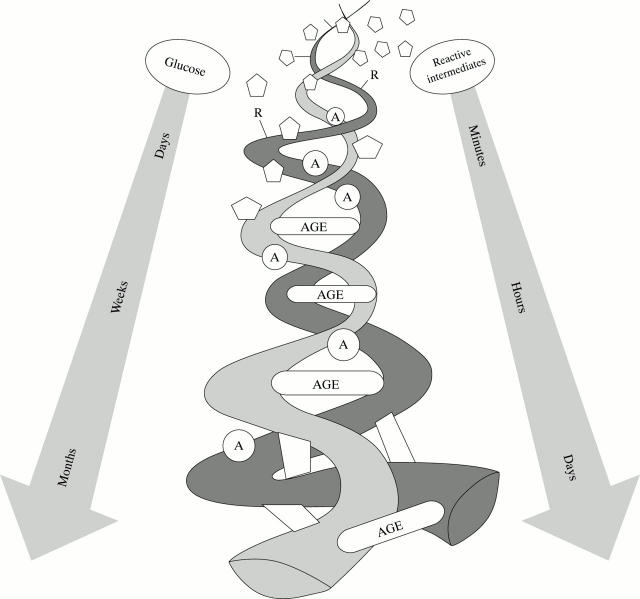
Schematic diagram illustrating the course of AGE formation on a hypothetical fibrilar protein. Open chain sugars or glycolytic intermediates (⬠) react with amino groups (R) to form Schiff bases and Amadori products (A) and eventually AGEs. Glucose may take several weeks to culminate in AGE formation leading to irreversible crosslink formation between protein fibrils or oxidative products. Reactive glycolytic intermediates such as methylglyoxal or 3-deoxyglucosone take much less time to form AGEs. Such AGE crosslinks can have a serious influence on protein structure and function.

Structures of advanced glycation end products.
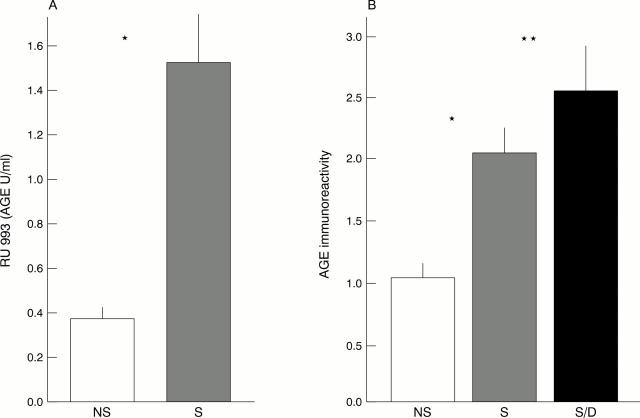
AGEs accumulate at high levels in the lens and coronary arteries of smokers. (A) The cataractous lenses of smokers (S) and non-smokers (NS) were removed, the protein extracted and quantified for AGE immunoreactivity using a competitive AGE-ELISA. AGE levels were significantly higher in the lenses of smokers (*p<0.0007) (Nicholl et al28). (B) AGE immunoreactivity in the vascular walls of coronary arteries from smokers, non-smokers, and smokers with diabetes. AGEs deposited at higher levels in patients with a history of smoking tobacco products. Significantly, patients who had diabetes and also smoked had supraelevated levels in their coronary arteries (*p<0.015; **p<0.001).
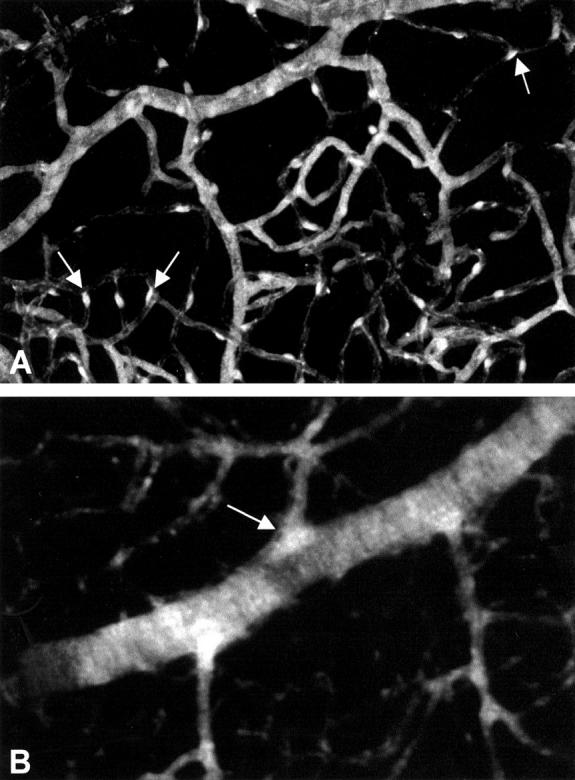
AGE immunoreactivity in diabetic and aged rats. (A) Trypsin digest of retinal vascular tree from an 8 month diabetic rat. AGE immunoreactivity is marked in the arterioles and capillaries. The pericytes of the retinal capillary beds are hyperfluorescent indicating accumulation of AGEs (arrows). (B) AGE immunoreactivity in the retinal vasculature of a 28 month old, non-diabetic rat. The immunofluorescence pattern is different from that observed in the diabetic retina (A) with AGE localisation appearing confined to the vascular basement membranes of arteries, arterioles and, to a lesser extent, the capillaries. Note the bright fluorescence at arteriolar sphincters (arrow).

AGEs and AGE receptor accumulation in lysosomes. (A) AGE receptor component (AGE-R1) (see Stitt et al33) immunoreactivity in a human RPE cell which was exposed to AGE albumin for 4 days before fixation. Note the hyperfluorescent areas in a perinuclear position—a distribution pattern which is indicative of RPE lysosomal compartments. (B) AGE immunoreactivity in a glomerular epithelial cell from a diabetic dog. Note the high density of gold particles in the lysosomes which indicate AGE accumulation in these organelles.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical