

A prospective comparison of simultaneous kidney-pancreas transplantation with systemic-enteric versus portal-enteric drainage
- PMID: 11371732
- PMCID: PMC1421316
- DOI: 10.1097/00000658-200106000-00003
A prospective comparison of simultaneous kidney-pancreas transplantation with systemic-enteric versus portal-enteric drainage
Abstract
Objective: To compare pancreas transplantation with systemic-enteric (SE) versus portal-enteric (PE) drainage in a prospective fashion.
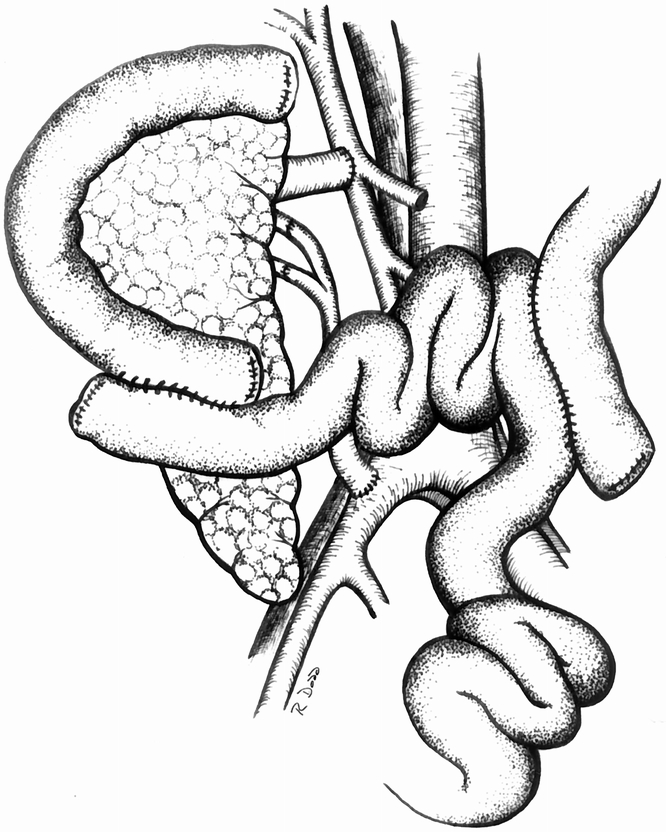
Summary background data: To improve the physiology of pancreas transplantation, the authors developed a new technique of portal venous delivery of insulin and enteric drainage of the exocrine secretions.
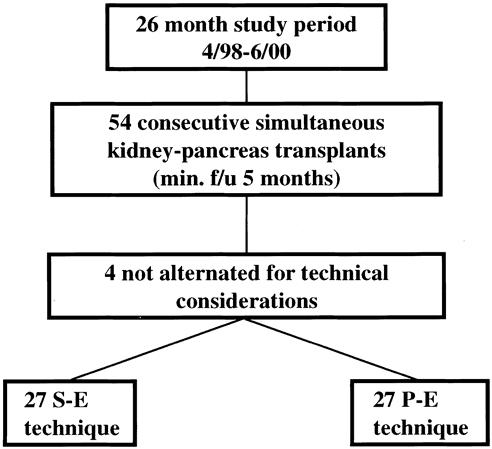
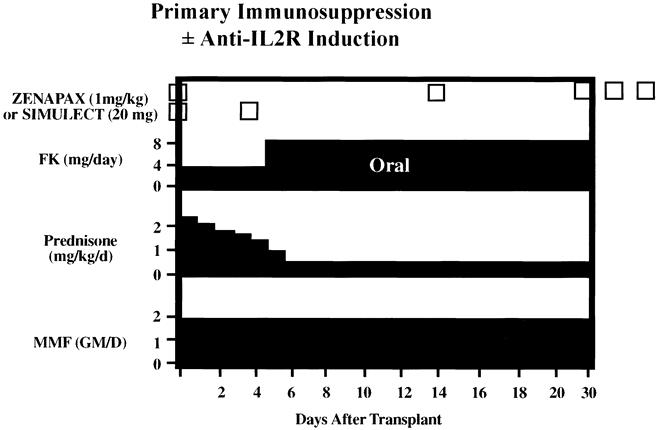
Methods: During a 26-month period, the authors prospectively alternated 54 consecutive simultaneous kidney and pancreas transplants to either SE (n = 27) or PE (n = 27) drainage. The two groups were well matched for numerous characteristics. Maintenance immunosuppression in both groups consisted of tacrolimus, mycophenolate mofetil, and steroids.
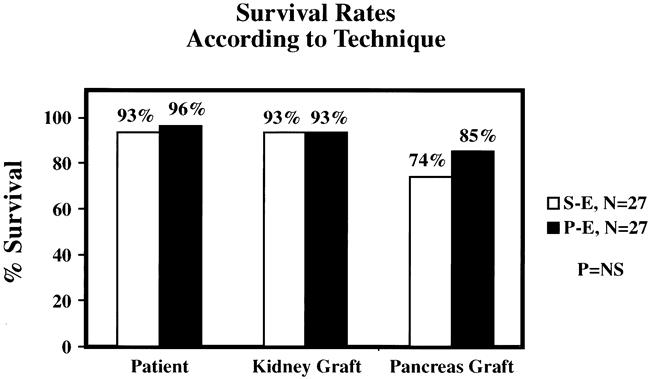
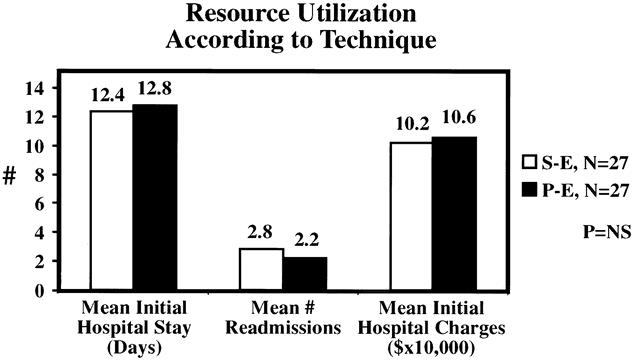
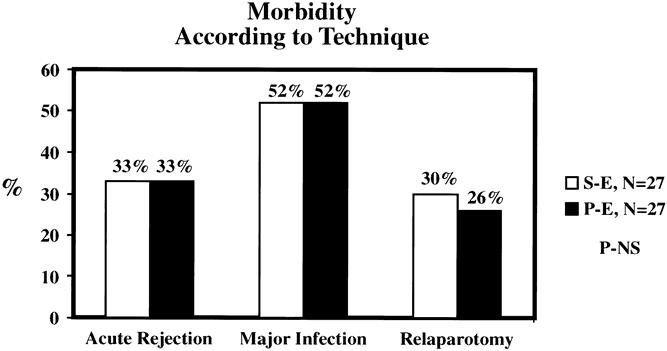
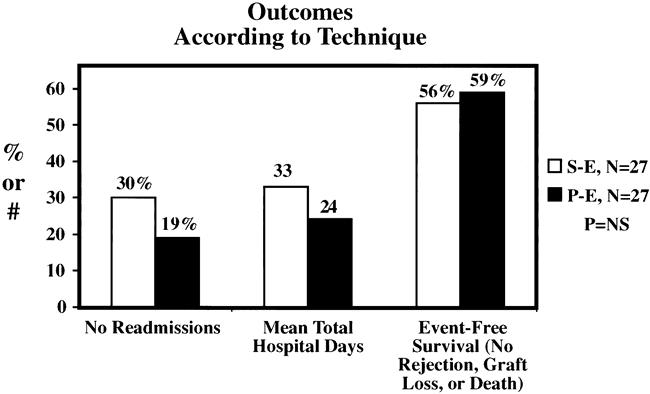
Results: Patient survival rates were 93% SE versus 96% PE; kidney graft survival rates were 93% in both groups. Pancreas transplantation survival (complete insulin independence) was 74% after SE versus 85% after PE drainage with a mean follow-up of 17 months. The mean length of initial hospital stay was 12.4 days in the SE group and 12.8 days in the PE group. The SE group was characterized by a slight increase in the number of readmissions. The incidences of acute rejection (33%) and major infection (52%) were similar in both groups. The incidence of intraabdominal infection was slightly higher in the SE group. However, the early relaparotomy rate was similar between groups. The composite endpoint of no rejection, graft loss, or death was attained in 56% of SE versus 59% of PE patients.
Conclusions: These results suggest that simultaneous kidney and pancreas transplantation with SE or PE drainage can be performed with comparable short-term outcomes.
Figures
References
-
- Sutherland DER, Gruessner AC. International Pancreas Transplant Registry update. IPTR Newsletter 2000; 12: 1–23.
-
- Gruessner AC, Sutherland DER. Analyses of pancreas transplant outcomes for United States cases reported to the United Network for Organ Sharing (UNOS) and non-US cases reported to the International Pancreas Transplant Registry (IPTR). In: Cecka JM, Terasaki PI, eds. Clinical transplants 1999. Los Angeles, CA: UCLA Immunogenetics Center; 2000: 51–69. - PubMed
-
- Shokouh-Amiri MH, Gaber AO, Gaber LW, et al. Pancreas transplantation with portal venous drainage and enteric exocrine diversion: a new technique. Transplant Proc 1992; 24: 776–777. - PubMed
-
- Gaber AO, Shokouh-Amiri H, Grewal HP, et al. A technique for portal pancreatic transplantation with enteric drainage. Surg Gynecol Obstet 1993; 177: 417–419. - PubMed
-
- Stratta RJ, Gaber AO, Shokouh-Amiri MH, et al. A prospective comparison of systemic-bladder versus portal-enteric drainage in vascularized pancreas transplantation. Surgery 2000; 127: 217–226. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
