

Homogeneity of antibody responses in tuberculosis patients
- PMID: 11402004
- PMCID: PMC98537
- DOI: 10.1128/IAI.69.7.4600-4609.2001
Homogeneity of antibody responses in tuberculosis patients
Abstract
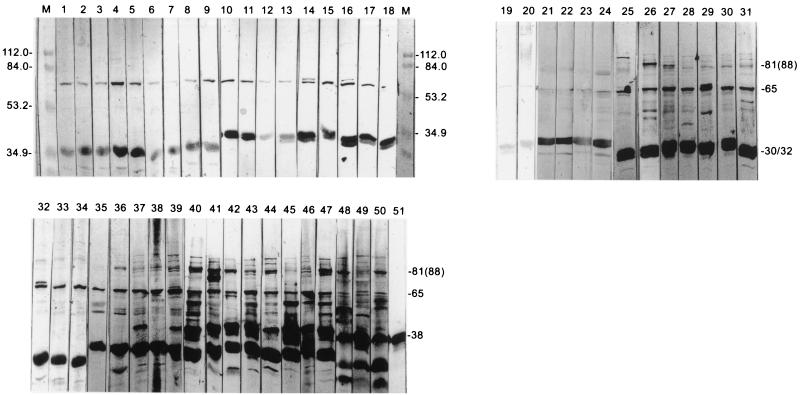
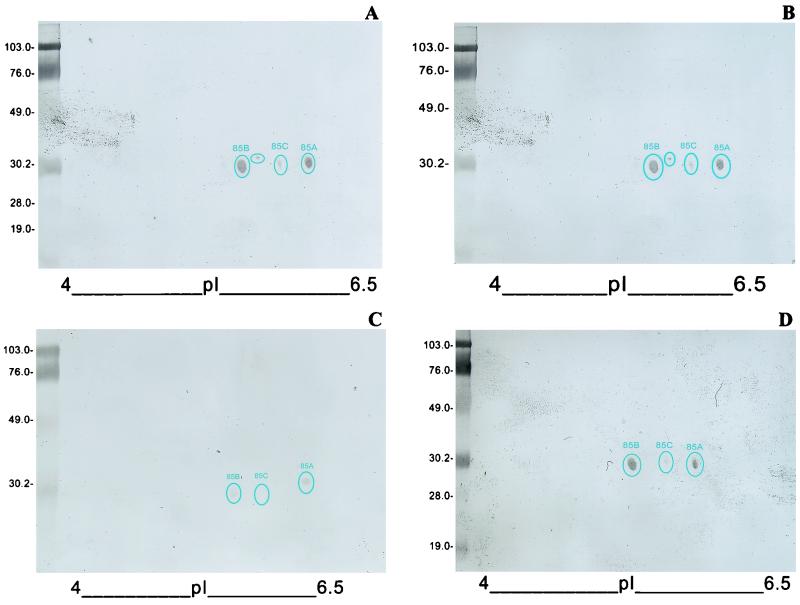
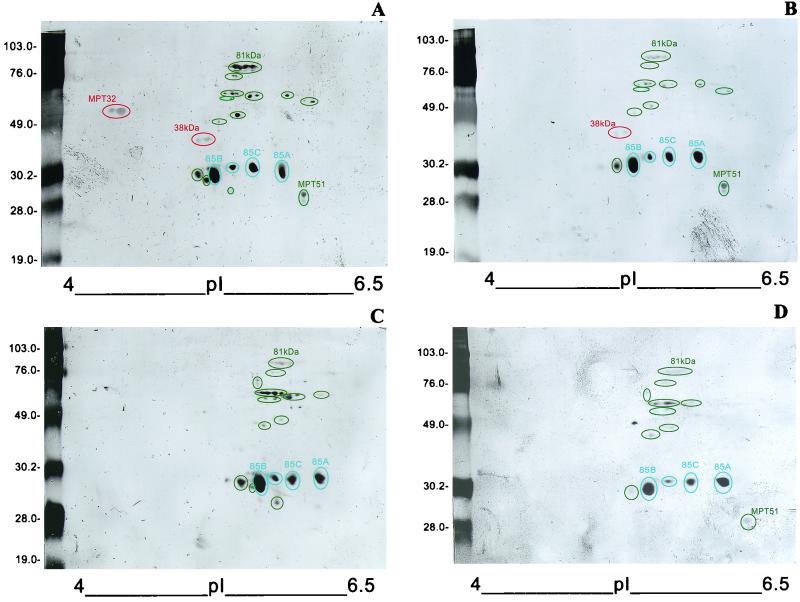
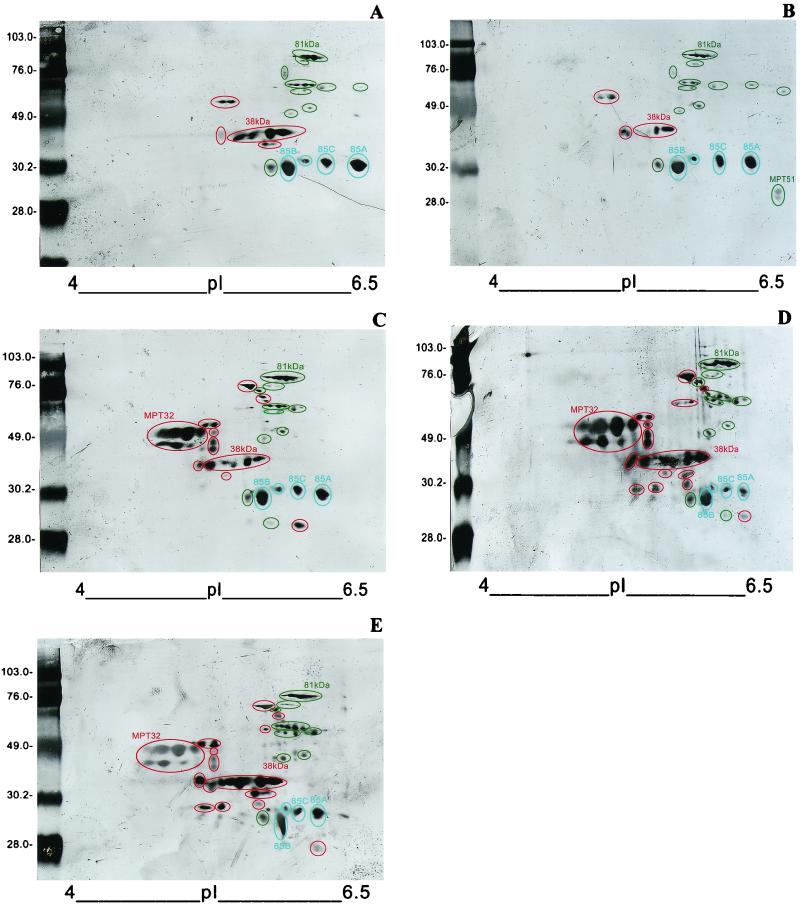
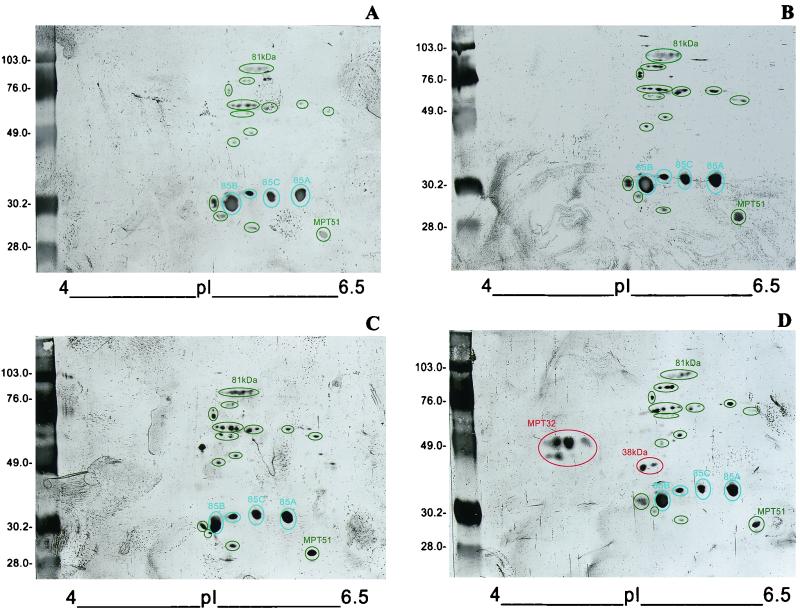
The goals of the present study were twofold: (i) to compare the repertoires of antigens in culture filtrates of in vitro-grown Mycobacterium tuberculosis that are recognized by antibodies from noncavitary and cavitary tuberculosis (TB) patients and (ii) to determine the extent of variation that exists between the antigen profiles recognized by individual TB patients. Lipoarabinomannan-free culture filtrate proteins of M. tuberculosis were fractionated by one-dimensional (1-D) and 2-D polyacrylamide gel electrophoresis, and the Western blots were probed with sera from non-human immunodeficiency virus (non-HIV)-infected cavitary and noncavitary TB patients and from HIV-infected, noncavitary TB patients. In contrast to earlier studies based on recombinant antigens of M. tuberculosis which suggested that antibody responses in TB patients were heterogeneous (K. Lyashchenko et al., 1998, Infect. Immun. 66:3936-3940, 1998), our studies with native culture filtrate proteins show that the antibody responses in TB patients show significant homogeneity in being directed against a well-defined subset of antigens. Thus, there is a well-defined subset of culture filtrate antigens that elicits antibodies during noncavitary and cavitary disease. In addition, another set of antigens is recognized primarily by cavitary TB patients. The mapping with individual patient sera presented here suggests that serodiagnostic tests based on the subset of antigens recognized during both noncavitary and cavitary TB will enhance the sensitivity of antibody detection in TB patients, especially in difficult-to-diagnose, smear-negative, noncavitary TB patients.
Figures
Similar articles
-
Delineation of human antibody responses to culture filtrate antigens of Mycobacterium tuberculosis.J Infect Dis. 1998 Nov;178(5):1534-8. doi: 10.1086/314438. J Infect Dis. 1998. PMID: 9780282
-
Serodiagnostic potential of culture filtrate antigens of Mycobacterium tuberculosis.Clin Diagn Lab Immunol. 2000 Jul;7(4):662-8. doi: 10.1128/CDLI.7.4.662-668.2000. Clin Diagn Lab Immunol. 2000. PMID: 10882669 Free PMC article.
-
Antigens of Mycobacterium tuberculosis recognized by antibodies during incipient, subclinical tuberculosis.Clin Diagn Lab Immunol. 2005 Feb;12(2):354-8. doi: 10.1128/CDLI.12.2.354-358.2005. Clin Diagn Lab Immunol. 2005. PMID: 15699433 Free PMC article.
-
Progress in serodiagnosis of Mycobacterium tuberculosis infection.Scand J Immunol. 2007 Aug-Sep;66(2-3):176-91. doi: 10.1111/j.1365-3083.2007.01978.x. Scand J Immunol. 2007. PMID: 17635795 Review.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
Cited by
-
Use of multiepitope polyproteins in serodiagnosis of active tuberculosis.Clin Diagn Lab Immunol. 2002 Jul;9(4):883-91. doi: 10.1128/cdli.9.4.883-891.2002. Clin Diagn Lab Immunol. 2002. PMID: 12093690 Free PMC article.
-
Immunodiagnosis of tuberculosis: a dynamic view of biomarker discovery.Clin Microbiol Rev. 2011 Oct;24(4):792-805. doi: 10.1128/CMR.00014-11. Clin Microbiol Rev. 2011. PMID: 21976609 Free PMC article. Review.
-
Comparative evaluation of profiles of antibodies to mycobacterial capsular polysaccharides in tuberculosis patients and controls stratified by HIV status.Clin Vaccine Immunol. 2012 Feb;19(2):198-208. doi: 10.1128/CVI.05550-11. Epub 2011 Dec 14. Clin Vaccine Immunol. 2012. PMID: 22169090 Free PMC article.
-
Performance of purified antigens for serodiagnosis of pulmonary tuberculosis: a meta-analysis.Clin Vaccine Immunol. 2009 Feb;16(2):260-76. doi: 10.1128/CVI.00355-08. Epub 2008 Dec 3. Clin Vaccine Immunol. 2009. PMID: 19052159 Free PMC article. Review.
-
LipC (Rv0220) is an immunogenic cell surface esterase of Mycobacterium tuberculosis.Infect Immun. 2012 Jan;80(1):243-53. doi: 10.1128/IAI.05541-11. Epub 2011 Oct 28. Infect Immun. 2012. PMID: 22038913 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
