

Permissive hypercapnia for the prevention of morbidity and mortality in mechanically ventilated newborn infants
- PMID: 11406029
- PMCID: PMC7017931
- DOI: 10.1002/14651858.CD002061
Permissive hypercapnia for the prevention of morbidity and mortality in mechanically ventilated newborn infants
Abstract
Background: Experimental animal data and uncontrolled, observational studies in human infants have suggested that hyperventilation and hypocapnia may be associated with increased pulmonary and neurodevelopmental morbidity. Protective ventilatory strategies allowing higher levels of arterial CO2 (permissive hypercapnia) are now widely used in adult critical care. The aggressive pursuit of normocapnia in ventilated newborn infants may contribute to the already present burden of lung disease. However, the safe or ideal range for PCO2 in this vulnerable population has not been established.
Objectives: To assess whether, in mechanically ventilated neonates, a strategy of permissive hypercapnia improves short and long term outcomes (esp. mortality, duration of respiratory support, incidence of chronic lung disease and neurodevelopmental outcome).
Search strategy: Standard strategies of the Cochrane Neonatal Review Group were used. Searches were made of the Oxford Database of Perinatal Trials, MEDLINE, CINAHL, and Current Contents. Searches were also made of previous reviews including cross-referencing, abstracts, and conference and symposia proceedings published in Pediatric Research.
Selection criteria: All randomised controlled trials in which a strategy of permissive hypercapnia was compared with conventional strategies aimed at achieving normocapnia (or lower levels of hypercapnia) in newborn infants who are mechanically ventilated were eligible.
Data collection and analysis: Standard methods of the Cochrane Neonatal Review Group were used. Trials identified by the search strategy were independently reviewed by each author and assessed for eligibility and trial quality. Data were extracted separately. Differences were compared and resolved. Additional information was requested from trial authors. Only published data were available for review. Results are expressed as relative risk and risk difference for dichotomous outcomes, and weighted mean difference for continuous variables.
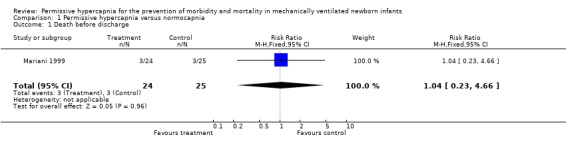
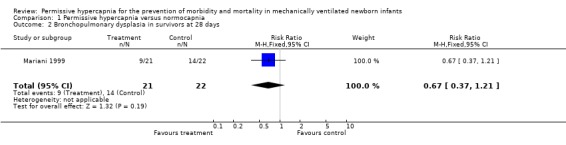
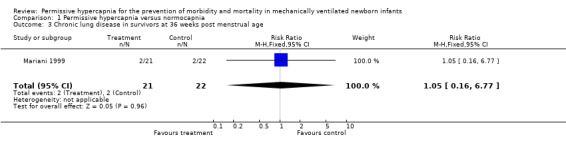
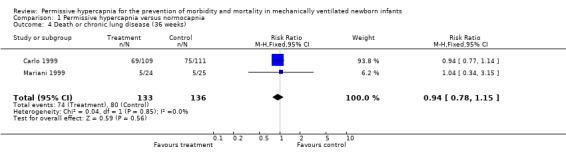
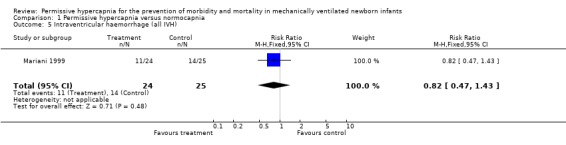
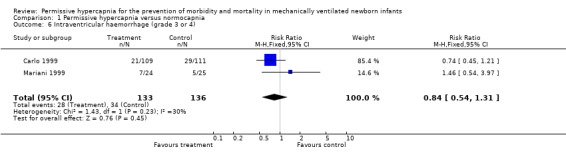
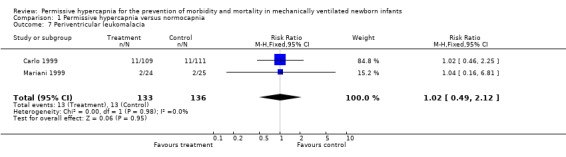
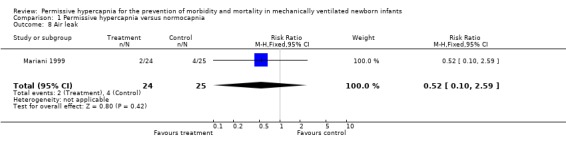
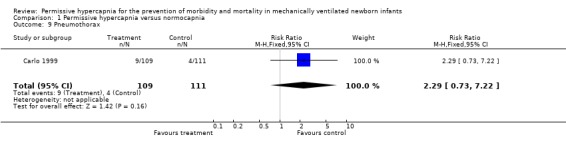
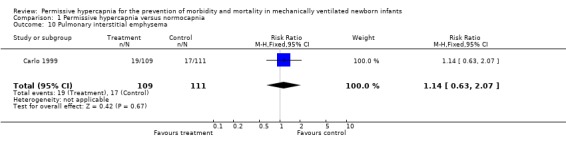
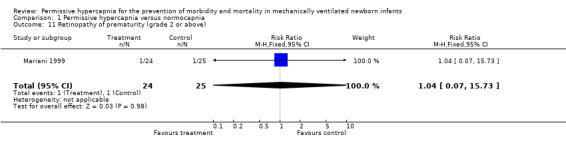
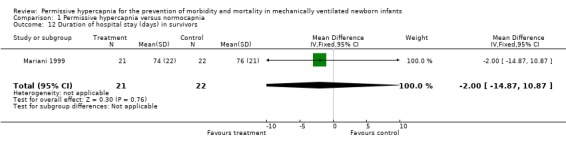
Main results: Two trials involving 269 newborn infants were included. Meta-analysis of combined data was possible for three outcomes. There was no evidence that permissive hypercapnia reduced the incidence of death or chronic lung disease at 36 weeks (RR 0.94, 95% CI 0.78, 1.15), intraventricular haemorrhage grade 3 or 4 (RR 0.84, 95% CI 0.54, 1.31) or periventricular leukomalacia (RR 1.02, 95% CI 0.49, 2.12). There were no differences in any other reported outcomes when the strategy of permissive hypercapnia/minimal ventilation was compared to routine ventilation in newborn infants. Long term neurodevelopmental outcomes were not reported. One trial reported that permissive hypercapnia reduced the incidence of chronic lung disease in the 501 to 750 gram subgroup.
Reviewer's conclusions: This review does not demonstrate any significant overall benefit of a permissive hypercapnia/minimal ventilation strategy compared to a routine ventilation strategy. At present, therefore, these ventilation strategies cannot be recommended to reduce mortality, or pulmonary and neurodevelopmental morbidity. Ventilatory strategies which target high levels of PCO2 (> 55 mmHg) should only be undertaken in the context of well-designed controlled clinical trials. These trials should aim to establish the safe, or ideal, range for CO2 in ventilated newborns, and examine the role of protective ventilatory techniques in achieving this target.
Conflict of interest statement
Nil
Figures
References
References to studies included in this review
Carlo 1999 {published data only}
-
- Carlo WA, Stark AR, Bauer C, Donovan E, Oh W, Papile L‐A, Shankaran S, Tyson JE, Wright LL, Temprosa, Poole K. Effects of minimal ventilation in a multicenter randomized controlled trial of ventilator support and early corticosteroid therapy in extremely low birthweight infants. Pediatrics 1999;104(3, Suppl):738‐39.
Mariani 1999 {published data only}
-
- Mariani G, Cifuentes J, Carlo WA. Randomized trial of permissive hypercapnia in preterm infants. Pediatrics 1999;104:1082‐8. - PubMed
References to studies awaiting assessment
Carlo 1999 (full) {published data only}
-
- Full report of Carlo 1999 expected in 2001.
Additional references
Amato 1998
-
- Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective‐ventilation strategy on mortality in the acute respiratory distress syndrome. New England Journal of Medicine 1998;338:347‐54. - PubMed
ARDS Network 2000
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine 2000;342:1301‐8. - PubMed
Avery 1987
-
- Avery ME, Tooley WH, Keller JB, et al. Is chronic lung disease in low birth weight infants preventable?: A survey of eight centers. Pediatrics 1987;79:26‐30. - PubMed
Bidani 1994
-
- Bidani A, Tzouanakis AE, Cardenas VJ, et al. Permissive hypercapnia in acute respiratory failure. JAMA 1994;272:957‐62. - PubMed
Calvert 1987
-
- Calvert SA, Hoskins EM, Fong KW, et al. Etiologic factors associated with the development of periventricular leukomalacia. Acta Paediatrica Scandinavica 1987;76:254‐9. - PubMed
Dreyfuss 1993
-
- Dreyfuss D, Sauman G. Role of tidal volume, FRC, and end‐expiratory volume in the development of pulmonary oedema following mechanical ventilation. American Review of Respiratory Disease 1993;148:1194‐203. - PubMed
Dries 1995
-
- Dries DJ. Permissive hypercapnia. Journal of Trauma 1995;39:984‐9. - PubMed
Drummond 1981
-
- Drummond WH, Gregory GA, Heyman MA, et al. The independent effects of hyperventilation, tolazoline, and dopamine on infants with persistent pulmonary hypertension. The Journal of Pediatrics 1981;98:603‐11. - PubMed
Feihl 1994
-
- Feihl F, Perret C. Permissive hypercapnia. How permissive should we be?. American Journal of Respiratory and Critical Care Medicine 1994;150:1722‐37. - PubMed
Ferrara 1984
-
- Ferrara B, Johnson DE, Change P‐N, et al. Efficacy and neurologic outcome of profound hypocapneic alkalosis for the treatment of persistent pulmonary hypertension in infancy. The Journal of Pediatrics 1984;105:457‐61. - PubMed
Fujimoto 1994
Garland 1995
-
- Garland JS, Buck RK, Allred EN, et al. Hypocarbia before surfactant therapy appears to increase bronchopulmonary dysplasia risk in infants with respiratory distress syndrome. Archives of Pediatrics and Adolescent Medicine 1995;149:617‐22. - PubMed
Graziani 1992
-
- Graziani LJ, Spitzer AR, Mitchell DG, et al. Mechanical ventilation in preterm infants: Neurosonographic and developmental studies. Pediatrics 1992;90:515‐22. - PubMed
Hendricks‐Munoz 1988
-
- Hendricks‐Munoz KD, Walton JP. Hearing loss in infants with persistent fetal circulation. Pediatrics 1988;81:650‐6. - PubMed
Kraybill 1989
-
- Kraybill EN, Runyan DK, Bose CL, et al. Risk factors for chronic lung disease in infants with birth weights of 751 to 1000 grams. The Journal of Pediatrics 1989;115:115‐20. - PubMed
Moylan 1978
-
- Moylan FM, Walker AM, Kramer SS, et al. Relationship of bronchopulmonary dysplasia to the occurrence of alveolar rupture during positive pressure ventilation. Critical Care Medicine 1978;6:140‐2. - PubMed
Northway 1967
-
- Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respiratory therapy of hyaline membrane disease: BPD. New England Journal of Medicine 1967;276:357‐68. - PubMed
Stewart 1998
-
- Stewart TE, Meade MO, Cook DJ, et al. Evaluation of a ventilation strategy to prevent barotrauma in patients at high risk for acute respiratory distress syndrome. New England Journal of Medicine 1998;338:355‐61. - PubMed
Tuxen 1994
-
- Tuxen DV. Permissive hypercapnic ventilation. American Journal of Respiratory and Critical Care Medicine 1994;150:870‐4. - PubMed
Wiswell 1996a
-
- Wiswell TE, Graziani LJ, Kornhauser MS, et al. Effects of hypocarbia on the development of cystic periventricular leukomalacia in premature infants treated with high‐frequency jet ventilation. Pediatrics 1996;98:918‐24. - PubMed
Wiswell 1996b
-
- Wiswell TE, Graziani LJ, Kornhauser MS, et al. High frequency jet ventilation in the early management of respiratory distress syndrome is associated with a greater risk for adverse outcomes. Pediatrics 1996;98:1035‐43. - PubMed
Wung 1985
-
- Wung J‐T, James LS, Kilchevsky E, et al. Management of infants with severe respiratory failure and persistence of the fetal circulation without hyperventilation. Pediatrics 1985;76:488‐94. - PubMed
Yu 1983
-
- Yu VY, Orgill AA, Lim SB, et al. Bronchopulmonary dysplasia in very low birthweight infants. Australian Paediatric Journal 1983;19:233‐6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources