

Randomised controlled trial of cardiotocography versus Doppler auscultation of fetal heart at admission in labour in low risk obstetric population
- PMID: 11408301
- PMCID: PMC32308
- DOI: 10.1136/bmj.322.7300.1457
Randomised controlled trial of cardiotocography versus Doppler auscultation of fetal heart at admission in labour in low risk obstetric population
Abstract
Objective: To compare the effect of admission cardiotocography and Doppler auscultation of the fetal heart on neonatal outcome and levels of obstetric intervention in a low risk obstetric population.
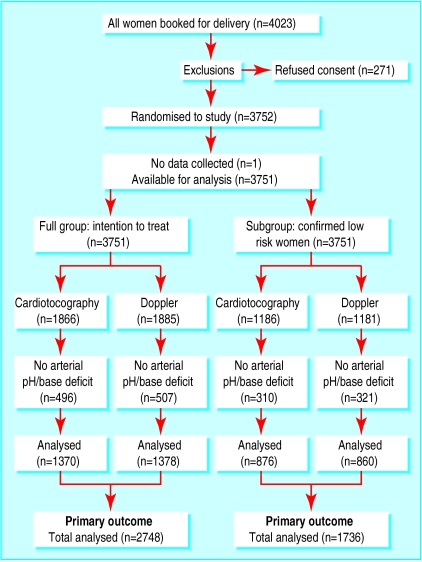
Design: Randomised controlled trial.
Setting: Obstetric unit of teaching hospital
Participants: Pregnant women who had no obstetric complications that warranted continuous monitoring of fetal heart rate in labour.
Intervention: Women were randomised to receive either cardiotocography or Doppler auscultation of the fetal heart when they were admitted in spontaneous uncomplicated labour.
Main outcome measures: The primary outcome measure was umbilical arterial metabolic acidosis. Secondary outcome measures included other measures of condition at birth and obstetric intervention.
Results: There were no significant differences in the incidence of metabolic acidosis or any other measure of neonatal outcome among women who remained at low risk when they were admitted in labour. However, compared with women who received Doppler auscultation, women who had admission cardiotocography were significantly more likely to have continuous fetal heart rate monitoring in labour (odds ratio 1.49, 95% confidence interval 1.26 to 1.76), augmentation of labour (1.26, 1.02 to 1.56), epidural analgesia (1.33, 1.10 to 1.61), and operative delivery (1.36, 1.12 to 1.65).
Conclusions: Compared with Doppler auscultation of the fetal heart, admission cardiotocography does not benefit neonatal outcome in low risk women. Its use results in increased obstetric intervention, including operative delivery.
Comment in
-
Electronic fetal monitoring. Is not necessary for low risk labours.BMJ. 2001 Jun 16;322(7300):1436-7. doi: 10.1136/bmj.322.7300.1436. BMJ. 2001. PMID: 11408285 Free PMC article. No abstract available.
-
Cardiotocography v Doppler auscultation. Guidelines highlight gaps in research evidence.BMJ. 2002 Feb 23;324(7335):482-5. BMJ. 2002. PMID: 11859056 Free PMC article. No abstract available.
-
Cardiotocography v Doppler auscultation. Conclusions do not recognise difference between statistical and clinical significance.BMJ. 2002 Feb 23;324(7335):483. BMJ. 2002. PMID: 11863005 No abstract available.
-
Cardiotocography v Doppler auscultation. All unbiased comparative studies should be published.BMJ. 2002 Feb 23;324(7335):483-5. BMJ. 2002. PMID: 11863006 No abstract available.
References
-
- Ingemarsson I. Electronic fetal monitoring as a screening test. In: Spencer JAD, Ward RHT, editors. Intrapartum fetal surveillance. London: Royal College of Obstetricians and Gynaecologists; 1993. pp. 45–52.
-
- Prentice A, Lind T. Fetal heart rate monitoring in labour—too frequent intervention, too little benefit? Lancet. 1997;ii:1375–1377. - PubMed
-
- Grant AM. Electronic fetal monitoring alone versus intermittent auscultation in labour. In: Enkin MW, Kierse MJNC, Renfrew MJ, Neilson JP, editors. Cochrane pregnancy and childbirth database. Oxford: Update Software; 1993.
-
- Thacker SB, Stroup DF, Peterson HB. Efficacy and safety of intrapartum electronic fetal monitoring: an update. Obstet Gynecol. 1995;86:613–620. - PubMed
-
- Thacker SB, Stroup DF. Continuous electronic heart rate monitoring for fetal assessment during labor Cochrane Database Syst Rev 2000;(2):CD000063. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources