

Case Reports
Cerebral amyloid angiopathy presenting as nonhemorrhagic diffuse encephalopathy: neuropathologic and neuroradiologic manifestations in one case
Affiliations
- PMID: 11415900
- PMCID: PMC7974807
Item in Clipboard
Case Reports
Cerebral amyloid angiopathy presenting as nonhemorrhagic diffuse encephalopathy: neuropathologic and neuroradiologic manifestations in one case
AJNR Am J Neuroradiol.
2001 Jun-Jul.
Abstract
A case of cerebral amyloid angiopathy is presented with MR imaging findings of high intense signal on T2-weighted sequences at the level of the white and gray matter of both hemispheres in the absence of neuroradiologic signs of cerebral hemorrhage. The biopsy specimen revealed deposition of amyloid in the walls of the intracranial arterial branches and focal ischemic changes and gliosis in the gray and white matter. We consider this presentation to be very unusual in patients affected by cerebral amyloid angiopathy.
Figures

Images obtained at the time of the first hospital admission. Axial view turbo spin-echo T2-weighted sequence. A, and B, Diffuse high intensity signal involving the cortex and the white matter of the right temporo-parieto-occipital region. Note also the involvement of the right frontal and left parieto-occipital regions. C, High intense signal can be seen in the occipital lobes bilaterally, involving both the gray and white matter.
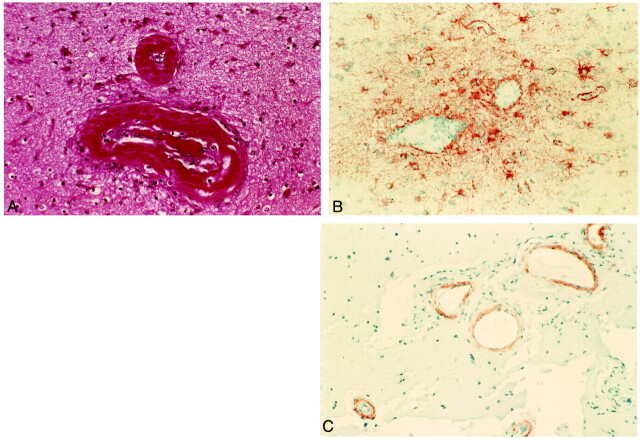
Histopathologic examinations of the lesions. A, Hematoxylin and eosin stain. Vessel walls are thickened by an amorphous eosinophilic substance, and the lumen of the vessel is partially occluded. B, Immunohistochemistry for glial fibrillary acidic protein shows perivascular gliosis. C, Immunohistochemistry for β-amyloid shows the presence of amyloid deposits in the vessel walls.
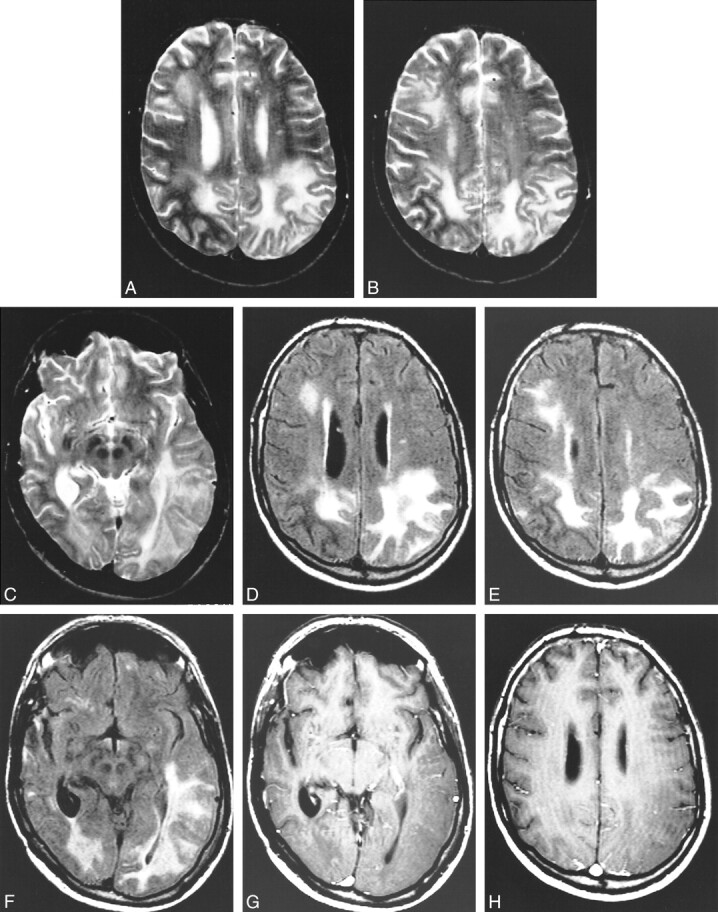
Images obtained at the 1-year follow-up examination. A, and B, Axial view spin-echo T2-weighted sequence. High intense signal is present in the gray and white matter of the right frontal lobe and of both parietal lobes. Note that compared with figure 1, there is progression of the disease in the left parietal lobe. The right parietal lobe, on the contrary, looks less involved. C, Axial view spin-echo T2-weighted sequence. The lesion on the left is involving also the temporal lobe. D, Axial view fluid-attenuated inversion recovery sequence obtained at the same level as that shown in A. The parietal lobes are diffusely hyperintense. High intensity signal is also present in the right frontal lobe. The right parietal lobe appears less involved than on the previous MR image. E, Axial view fluid-attenuated inversion recovery sequence obtained at the same level as that shown in B. The parietal lobes are diffusely hyperintense. High intensity signal is also present in the right frontal lobe. The right parietal lobe appears less involved than on the previous MR image. F, Axial view fluid-attenuated inversion recovery sequence obtained at the same level as that shown in C. The parietal lobes are diffusely hyperintense. High intensity signal is also present in the right frontal lobe. The right parietal lobe appears less involved than on the previous MR image. G, Infused axial view spin-echo T1-weighted sequence. There is no evidence of abnormal contrast enhancement in the diseased regions. H, Infused axial view spin-echo T1-weighted sequences. There is no evidence of abnormal contrast enhancement in the diseased regions.
Similar articles
-
Encephalopathy with amyloid angiopathy and numerous amyloid plaques with low levels of CSF Aβ1-40/Aβ1-42.Amyloid. 2012 Dec;19(4):186-90. doi: 10.3109/13506129.2012.725113. Epub 2012 Sep 21. Amyloid. 2012. PMID: 22994303
-
Cerebral amyloid angiopathy mimicking central nervous system metastases: a case report.J Med Case Rep. 2018 May 14;12(1):133. doi: 10.1186/s13256-018-1655-6. J Med Case Rep. 2018. PMID: 29754590 Free PMC article.
-
Spontaneous intracerebral hemorrhage secondary to cerebral amyloid angiopathy.J Am Geriatr Soc. 2009 Sep;57(9):1714-6. doi: 10.1111/j.1532-5415.2009.02403.x. J Am Geriatr Soc. 2009. PMID: 19895438 No abstract available.
-
[Cerebral amyloid angiopathy].Psychol Neuropsychiatr Vieil. 2007 Mar;5(1):35-45. Psychol Neuropsychiatr Vieil. 2007. PMID: 17412664 Review. French.
-
The Inflammatory Form of Cerebral Amyloid Angiopathy or "Cerebral Amyloid Angiopathy-Related Inflammation" (CAARI).Curr Neurol Neurosci Rep. 2015 Aug;15(8):54. doi: 10.1007/s11910-015-0572-y. Curr Neurol Neurosci Rep. 2015. PMID: 26096511 Review.
Cited by
-
When Atrial Fibrillation Meets Cerebral Amyloid Angiopathy: Current Evidence and Strategies.J Clin Med. 2023 Dec 15;12(24):7704. doi: 10.3390/jcm12247704. J Clin Med. 2023. PMID: 38137773 Free PMC article. Review.
-
Pseudotumoral Presentation of Cerebral Amyloid-Beta Angiopathy: Case Report and Review of Literature.Psychiatry Investig. 2021 Jun;18(6):479-485. doi: 10.30773/pi.2020.0201. Epub 2021 Jun 17. Psychiatry Investig. 2021. PMID: 34130443 Free PMC article.
References
-
- Oppenheimen G. Uber drusige nekrozen in der grosshirnrinde. Neurol Centralbi 1909;28:410-413
-
- Bruni J, Bilbao JM, Pritzker KP. Vascular amyloid in the aging CNS: clinicopathological study and literature review. Can J Neurol Sci 1977;4:239-244 - PubMed
-
- Vanley CT, Aguilar MJ, Kleinhenz RJ, Lagios MD. Cerebral amyloid angiopathy. Hum Pathol 1981;12:609-619 - PubMed
-
- Okazaki H, Reagan TJ, Campbell RJ. Clinicopathological studies of primary cerebral amyloid angiopathy. Mayo Clin Proc 1979;54:22-31 - PubMed
-
- Cohen M, Lanska D. Amyloidoma of the CNS: I. clinical and pathologic study. Neurology 1992;42:2019-2023 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical