

Quantitative MR evaluation of intracranial epidermoid tumors by fast fluid-attenuated inversion recovery imaging and echo-planar diffusion-weighted imaging
- PMID: 11415903
- PMCID: PMC7974800
Quantitative MR evaluation of intracranial epidermoid tumors by fast fluid-attenuated inversion recovery imaging and echo-planar diffusion-weighted imaging
Abstract
Background and purpose: Quantification of MR can provide objective, accurate criteria for evaluation of a given MR sequence. We quantitatively compared conventional MR sequences with fast fluid-attenuated inversion recovery (fast-FLAIR) and echo-planar diffusion-weighted (DW) MR imaging in the examination of intracranial epidermoid tumors.
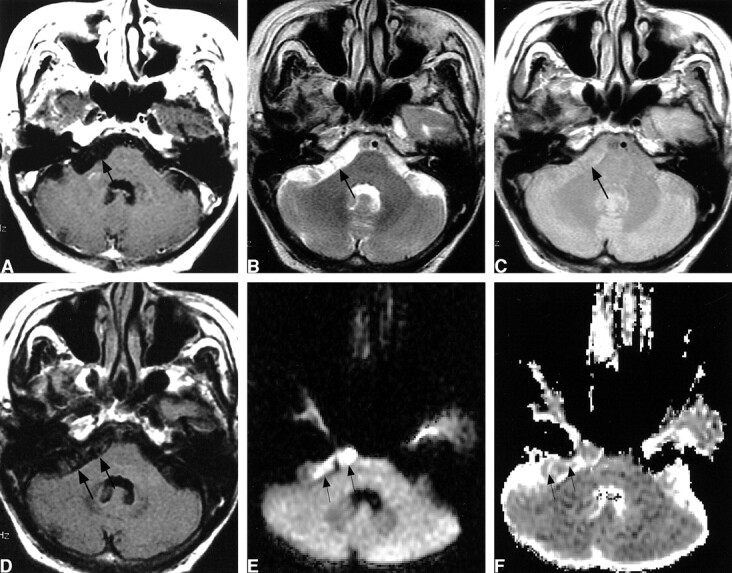
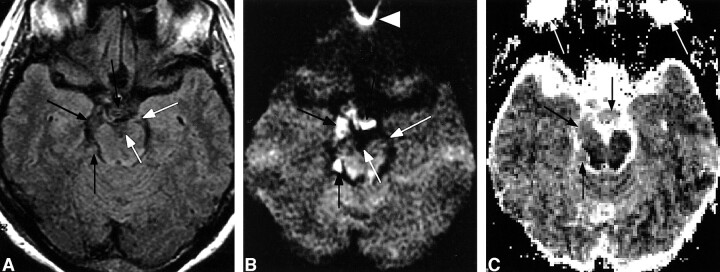
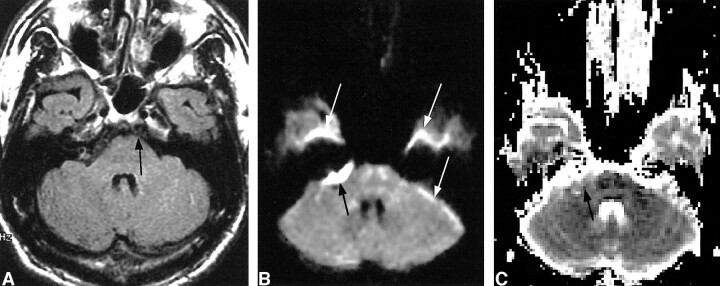
Methods: Eight patients with surgically confirmed intracranial epidermoid tumors were examined with T1-weighted MR sequences, fast T2- and proton density-weighted dual-echo sequences, fast-FLAIR sequences, and DW echo-planar sequences. We measured the MR signal intensity and apparent diffusion coefficient (ADC) of epidermoid tumors, normal brain tissue, and CSF and calculated the tumor-to-brain and tumor-to-CSF contrast ratios and contrast-to-noise ratios (CNR). Results were compared among the five MR methods.
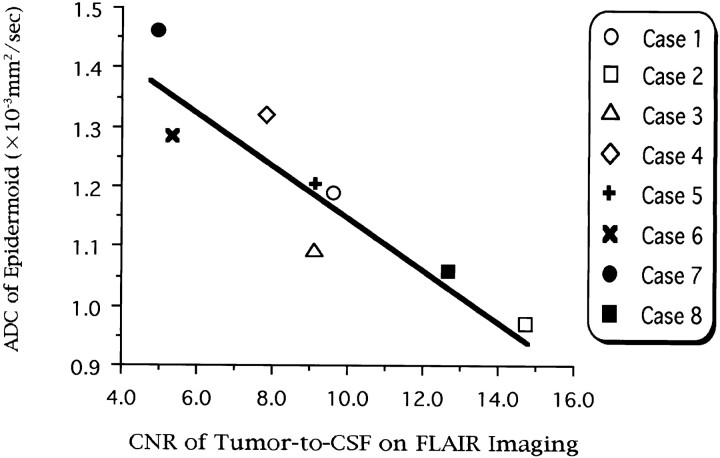
Results: On fast-FLAIR imaging, the mean signal intensity of epidermoid tumors was significantly higher than that of CSF but significantly lower than that of the brain; the contrast ratio and CNR of tumor-to-CSF were 4.71 and 9.17, respectively, significantly greater than the values with conventional MR imaging. On echo-planar DW imaging, epidermoid tumors showed a remarkably hyperintense signal relative to those of the brain and CSF; the mean contrast ratio and CNR of tumor-to-CSF were 13.25 and 19.34, respectively, significantly greater than those on fast-FLAIR or conventional MR imaging. The mean ADC of epidermoid tumors was 1.197 x 10(-3) mm(2)/s, significantly lower than that of CSF but higher than that of brain tissues.
Conclusion: Fast-FLAIR imaging is superior to conventional MR imaging in depicting intracranial epidermoid tumors. Echo-planar DW imaging provides the best lesion conspicuity among the five MR methods. The hyperintensity of epidermoid tumors on echo-planar DW imaging is not caused by the diffusion restriction but by the T2 shine-through effect.
Figures
References
-
- Conley FK. Epidermoid and dermoid tumors: clinical features and surgical management. In: Wilkins RH, Rengachary SS, eds. Neurosurgery 2nd ed. New York, NY: McGraw-Hill, Health Professions Division; 1996;971–976
-
- Vion-Dury J, Vincentelli F, Jiddane M, et al. MR imaging of epidermoid cysts. Neuroradiology 1987;29:333-338 - PubMed
-
- Yasargil MG, Abernathey CD, Sarioglu AC. Microneurosurgical treatment of intracranial dermoid and epidermoid tumors. Neurosurgery 1989;24:561-567 - PubMed
-
- Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Neurosurgery 1989;24:568-573 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical