

Dynamic contrast-enhanced T2*-weighted MR imaging of tumefactive demyelinating lesions
- PMID: 11415906
- PMCID: PMC7974773
Dynamic contrast-enhanced T2*-weighted MR imaging of tumefactive demyelinating lesions
Abstract
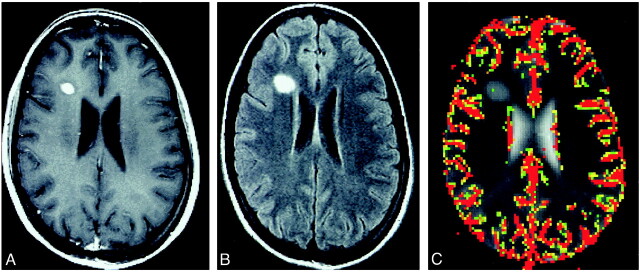
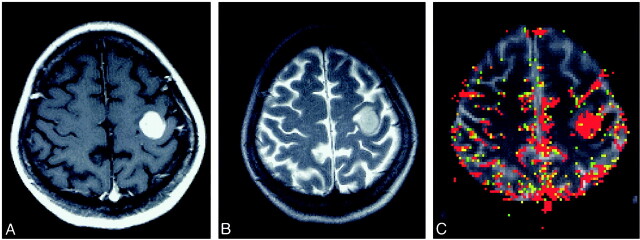
Purpose: Dynamic contrast-enhanced T2*-weighted MR imaging has been helpful in characterizing intracranial mass lesions by providing information on vascularity. Tumefactive demyelinating lesions (TDLs) can mimic intracranial neoplasms on conventional MR images, can be difficult to diagnose, and often result in surgical biopsy for suspected tumor. The purpose of this study was to determine whether dynamic contrast-enhanced T2*-weighted MR imaging can be used to distinguish between TDLs and intracranial neoplasms that share common features on conventional MR images.
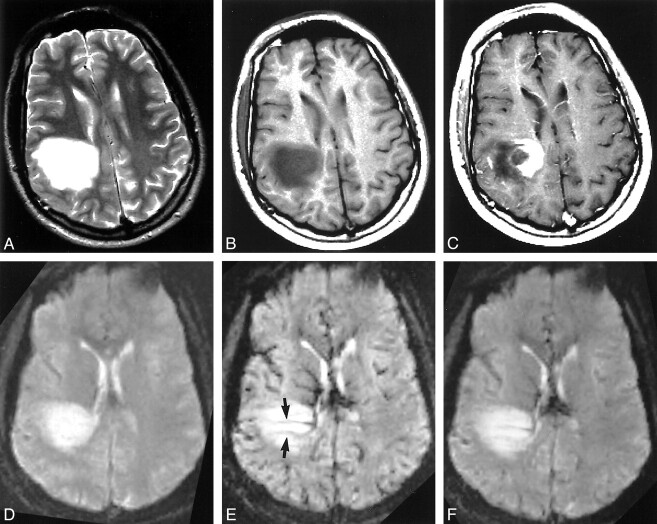
Methods: We retrospectively reviewed the conventional and dynamic contrast-enhanced T2*-weighted MR images and medical records of 10 patients with tumefactive demyelinating disease that was diagnosed by either biopsy or strong clinical suspicion supported by laboratory evaluation that included CSF analysis and evoked potential tests. Twelve TDLs in 10 patients and 11 brain tumors that appeared similar on conventional MR images were studied. Relative cerebral blood volume (rCBV) was calculated from dynamic MR data and was expressed as a ratio to contralateral normal white matter. rCBV values from 11 patients with intracranial neoplasms with very similar conventional MR imaging features were used for comparison.
Results: The rCBV values of TDLs ranged from 0.22 to 1.79 (n = 12), with a mean of 0.88 +/- 0.46 (SD). The rCBV values of intracranial neoplasms ranged from 1.55 to 19.20 (n = 11), with a mean of 6.47 +/- 6.52. The difference in rCBV values between the two groups was statistically significant (P =.009). The difference in rCBV values between TDLs and primary cerebral lymphomas (n = 4) was less pronounced but was statistically significant (P =.005).
Conclusion: Dynamic contrast-enhanced T2*-weighted MR imaging is a useful diagnostic tool in differentiating TDLs from intracranial neoplasms and may therefore obviate unnecessary surgical biopsy.
Figures
References
-
- Zagzag D, Miller DC, Kleinman GM, Abati A, Donnenfeld H, Budzilovich GN. Demyelinating disease versus tumor in surgical neuropathology: clues to a correct pathological diagnosis. Am J Surg Pathol 1993;17:537-545 - PubMed
-
- Hunter SB, Ballinger WE Jr, Rubin JJ. Multiple sclerosis mimicking primary brain tumor. Arch Pathol Lab Med 1987;111:464-468 - PubMed
-
- Giang DW, Poduri KR, Eskin TA, et al. Multiple sclerosis masquerading as a mass lesion. Neuroradiology 1992;34:150-154 - PubMed
-
- Prineas JW, McDonald WI. Demyelinating diseases. Greenfield's Neuropathology. ed 6. vol I. New York: Wiley; 1997:814–846
-
- Kepes JJ. Large focal tumor-like demyelinating lesions of the brain: intermediate entity between multiple sclerosis and acute disseminated encephalomyelitis? a study of 31 patients. Ann Neurol 1993;33:18-27 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical