

Patient evaluation and management with selective use of magnetic resonance cholangiography and endoscopic retrograde cholangiopancreatography before laparoscopic cholecystectomy
- PMID: 11420481
- PMCID: PMC1421945
- DOI: 10.1097/00000658-200107000-00006
Patient evaluation and management with selective use of magnetic resonance cholangiography and endoscopic retrograde cholangiopancreatography before laparoscopic cholecystectomy
Abstract
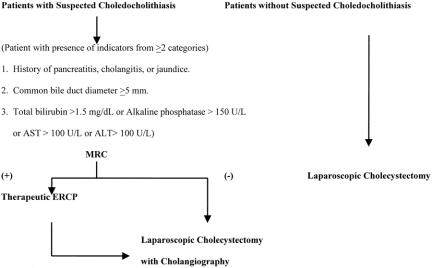
Objective: To assess the utility of triage guidelines for patients with cholelithiasis and suspected choledocholithiasis, incorporating selective use of magnetic resonance cholangiography (MRC) and endoscopic retrograde cholangiopancreatography (ERCP) before laparoscopic cholecystectomy (LC).
Summary background data: ERCP is the most frequently used modality for the diagnosis and resolution of choledocholithiasis before LC. MRC has recently emerged as an accurate, noninvasive modality for the detection of choledocholithiasis. However, useful strategies for implementing this diagnostic modality for patient evaluation before LC have not been investigated.
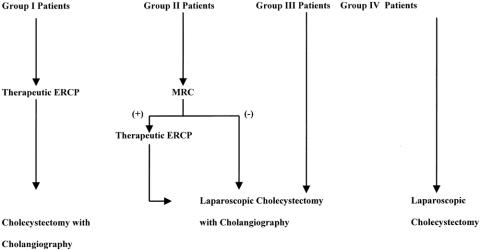
Methods: During a 16-month period, the authors prospectively evaluated all patients before LC using triage guidelines incorporating patient information obtained from clinical evaluation, serum chemistry analysis, and abdominal ultrasonography. Patients were then assigned to one of four groups based on the level of suspicion for choledocholithiasis (group I, extremely high; group 2, high; group 3, moderate; group 4, low). Group 1 patients underwent ERCP and clearance of common bile duct stones; group 2 patients underwent MRC; group 3 patients underwent LC with intraoperative cholangiography; and group 4 patients underwent LC without intraoperative cholangiography.
Results: Choledocholithiasis was detected in 43 of 440 patients (9.8%). The occurrence of choledocholithiasis among patients in the four groups were 92.6% (25/27), 32.4% (12/37), 3.8% (2/52), and 0.9% (3/324) for groups 1, 2, 3, and 4, respectively (P <.001). MRC was used for 8.4% (37/440) of patients. Patient triage resulted in the identification of common bile duct stones during preoperative ERCP in 92.3% (36/39) of the patients. Unsuspected common bile duct stones occurred in six patients (1.4%).
Conclusions: The probability of choledocholithiasis can be accurately assessed based on information obtained during the initial noninvasive evaluation. Stratification of risks for choledocholithiasis facilitates patient management with the most appropriate diagnostic studies and interventions, thereby improving patient care and resource utilization.
Figures
Comment in
-
Patient evaluation and management with selective use of magnetic resonance cholangiography (MRC) and endoscopic retrograde cholangiopancreatography (ERCP) before laparoscopic cholecystectomy (LC).Ann Surg. 2002 Nov;236(5):696; author reply 696-7. doi: 10.1097/01.SLA.0000037257.69656.6F. Ann Surg. 2002. PMID: 12409678 Free PMC article. No abstract available.
References
-
- Diel AK. Epidemiology and natural history of gallstone disease. Gastroenterol Clin North Am 1991; 20: 1–19. - PubMed
-
- Koo KP, Traverso LW. Do predictive indicators predict the presence of common bile duct stones during laparoscopic cholecystectomy? Am J Surg 1996; 171: 495–499. - PubMed
-
- Alponat A, Kum K, Rajnakova A, et al. Predictive factors for synchronous common bile duct stones in patients with choledocholithiasis. Surg Endosc 1997; 11: 928–932. - PubMed
-
- Trondsen E, Edwin B, Reiertsen O, et al. Prediction of common bile duct stones prior to cholecystectomy. A prospective validation of a discriminant analysis function. Arch Surg 1998; 133: 162–166. - PubMed
-
- Paul A, Milat B, Holthausen U, et al. Diagnosis and treatment of common bile duct stones (CBDS). Result of a consensus development conference. Surg Endosc 1998; 12: 856–864. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
